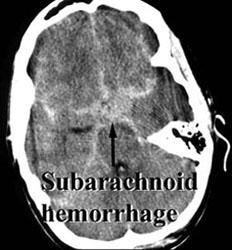
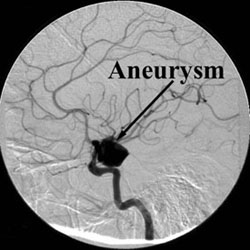
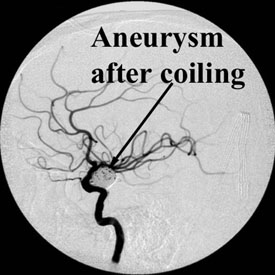
Coil Embolization of Aneurysm
Aneurysms may be treated by placing detachable platinum coils inside the aneurysm. The goal of the endovascular treatment is to pack the aneurysm tightly to close off blood flow into the aneurysm thereby preventing its rupture, or to reduce mass effect.
If interested in this procedure contact the Division of Diagnostic and Interventional Neuroradiology.
Henry Z. Wang, M.D., Ph.D.
P-L Westesson, M.D., Ph.D., D.D.S.
Department of Radiology - PO Box 648
University of Rochester Medical Center
601 Elmwood Avenue
Rochester, NY 14642-8648
Telephone: (585) 275-1839
Fax:(585) 473-4861
henry_wang@urmc.rochester.edu
perlennart_westesson@urmc.rochester.edu
Articles
Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, Sandercock P; International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomized comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005 Sep 3-9;366(9488):809-17. [PubMed]
ABSTRACT:
BACKGROUND: Two types of treatment are being used for patients with ruptured intracranial aneurysms: endovascular detachable-coil treatment or craniotomy and clipping. We undertook a randomized, multicentre trial to compare these treatments in patients who were suitable for either treatment because the relative safety and efficacy of these approaches had not been established. Here we present clinical outcomes 1 year after treatment. METHODS: 2143 patients with ruptured intracranial aneurysms, who were admitted to 42 neurosurgical centres, mainly in the UK and Europe, took part in the trial. They were randomly assigned to neurosurgical clipping (n=1070) or endovascular coiling (n=1073). The primary outcome was death or dependence at 1 year (defined by a modified Rankin scale of 3-6). Secondary outcomes included rebleeding from the treated aneurysm and risk of seizures. Long-term follow up continues. Analysis was in accordance with the randomized treatment. FINDINGS: We report the 1-year outcomes for 1063 of 1073 patients allocated to endovascular treatment, and 1055 of 1070 patients allocated to neurosurgical treatment. 250 (23.5%) of 1063 patients allocated to endovascular treatment were dead or dependent at 1 year, compared with 326 (30.9%) of 1055 patients allocated to neurosurgery, an absolute risk reduction of 7.4% (95% CI 3.6-11.2, p=0.0001). The early survival advantage was maintained for up to 7 years and was significant (log rank p=0.03). The risk of epilepsy was substantially lower in patients allocated to endovascular treatment, but the risk of late rebleeding was higher. INTERPRETATION: In patients with ruptured intracranial aneurysms suitable for both treatments, endovascular coiling is more likely to result in independent survival at 1 year than neurosurgical clipping; the survival benefit continues for at least 7 years. The risk of late rebleeding is low, but is more common after endovascular coiling than after neurosurgical clipping.
Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, Forbes GS, Thielen K, Nichols D, O'Fallon WM, Peacock J, Jaeger L, Kassell NF, Kongable-Beckman GL, Torner JC; International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003 Jul 12;362(9378):103-10. [PubMed]
ABSTRACT:
BACKGROUND: The management of unruptured intracranial aneurysms is controversial. Investigators from the International Study of Unruptured Intracranial Aneurysms aimed to assess the natural history of unruptured intracranial aneurysms and to measure the risk associated with their repair. METHODS: Centres in the USA, Canada, and Europe enrolled patients for prospective assessment of unruptured aneurysms. Investigators recorded the natural history in patients who did not have surgery, and assessed morbidity and mortality associated with repair of unruptured aneurysms by either open surgery or endovascular procedures. FINDINGS: 4060 patients were assessed-1692 did not have aneurysmal repair, 1917 had open surgery, and 451 had endovascular procedures. 5-year cumulative rupture rates for patients who did not have a history of subarachnoid hemorrhage with aneurysms located in internal carotid artery, anterior communicating or anterior cerebral artery, or middle cerebral artery were 0%, 2. 6%, 14.5%, and 40% for aneurysms less than 7 mm, 7-12 mm, 13-24 mm, and 25 mm or greater, respectively, compared with rates of 2.5%, 14.5%, 18.4%, and 50%, respectively, for the same size categories involving posterior circulation and posterior communicating artery aneurysms. These rates were often equalled or exceeded by the risks associated with surgical or endovascular repair of comparable lesions. Patients' age was a strong predictor of surgical outcome, and the size and location of an aneurysm predict both surgical and endovascular outcomes. INTERPRETATION: Many factors are involved in management of patients with unruptured intracranial aneurysms. Site, size, and group specific risks of the natural history should be compared with site, size, and age-specific risks of repair for each patient.
Back to list of procedures