HER2 FISH Testing for Breast Cancer
Complete Breast and Gastric Cancer Care
Better testing. Better patient outcomes.
Working with our dedicated and highly trained Surgical Pathology Team at UR Medicine Labs means that you will receive quicker turnaround for results and personal attention to your cases. You can be assured that you are getting the best in clinical laboratory testing such as:
- Sub-specialty surgical pathologists that read each case and are available for one-on-one discussion
- Latest in breast and gastric cancer testing
- Faster results (24-48 hour turnaround time)
- Lower cost associated with onsite testing
- Testing rigorously validated according to ASCO/CAP guidelines
- Testing performed in a facility that strictly follows ASCO/CAP guidelines for specimen handling
- FDA approved test kits are used for determining the HER2 status and eligibility for HER2-targeted therapy
Proper results determine the course of therapy for Breast and Gastric Cancer patients. Patients’ tumors that test equivocal for HER2 IHC need further testing to confirm HER2 status.
Breast Panel
- Estrogen Receptor (ER) and Progesterone Receptor (PR)
- HER2 IHC and HER2 FISH
Gastric Panel



Figure 1 legend: Immunohistochemistry utilizes antibodies against HER2 to assess the level of protein expression at the membrane of invasive tumor cells in formalin fixed paraffin embedded sections (DAKO Hercep Test, x400 original magnification). The interpretation of HER2 results must be semi-quantitatively evaluated in order to be useful for treatment planning.
(A) Breast tumors with either absent or partial weak membrane staining will typically demonstrate a normal HER2 gene status by FISH and are considered HER2 negative (scored as 0 or 1+). These patients are unlikely to benefit from HER2-targeted therapy.
(B) Breast tumors with evidence of circumferential membrane staining that is either weak or heterogeneous in its distribution (< 10% of tumor cells) should be scored as equivocal (scored as 2+). This pattern of staining has shown poor concordance with the HER2 gene status by FISH and is considered inconclusive. Breast tumors with an equivocal HER2 IHC result need to undergo reflex testing by FISH to resolve the HER2 status, allowing clinical decisions to be made about adjuvant treatment. Breast cancers with diffuse intense circumferential membrane staining (so called “chicken-wire” pattern) in >10% of invasive tumor cells.
(C) Should be considered HER2 positive by IHC. Tumors with this staining pattern show a good concordance with HER2 gene amplification by FISH in the majority of cases and will be the most likely to benefit from HER2 targeted therapy.



Figure 2 legend: Fluorescence in situ hybridization (FISH) assay for HER2 quantitatively measures the level of HER2 gene amplification in breast cancer tumor cell nuclei. This image shows the appearance of the dual-colored FISH assay (DAKO HER2 FISH pharmDXTM, x1000 original magnification). Invasive tumor cell nuclei are highlighted by the blue fluorescent counter stain (4’,6-diamidino-2-phenylindole [DAPI]).
(A) Shows non-amplified breast cancer with roughly equal numbers of HER2 (red signals) and CEP17 (green signals) with a calculated HER2/CEP17 ratio of less than 2.0. These patients are unlikely to benefit from HER2-targeted therapy.
(B) Shows FISH equivocal breast cancer were the average HER2 copy number is increased (> 4 but < 6) with a calculated HER2/CEP17 ratio of < 2. An equivocal FISH result requires additional testing (HER2 IHC, testing another block from the patients tumor, repeat FISH with an alternative chromosome 17 reference probe) to try and resolve the HER2 status for clinical decisions on adjuvant treatment.
(C) Shows HER2-amplified breast cancer with an increased number of HER2 gene signals (red signals) relative to CEP17 (green signals) resulting in a calculated HER2/CE17 ration of greater than 2. These patients will be the most likely to benefit from HER2 targeted therapy.
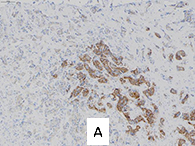

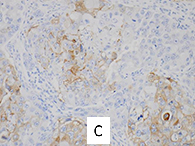
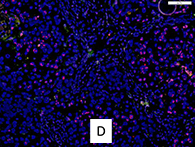
Figure 3 legend: The majority of tumors that demonstrate HER2 gene amplification/protein over-expression show this alteration diffusely throughout all areas of the invasive tumor. Occasionally, one encounters heterogeneity of gene amplification with clusters of cells with HER2 over-expression/amplification amid cells with a normal HER2 protein and gene status within the same or different regions of a single tumor. The term ‘HER2 intratumoral-heterogeneity’ or genomic heterogeneity has been used to describe this coexistence of multiple tumor cell subpopulations with distinctive HER2 amplification/over-expression characteristics within the same cancer. These changes can be observed at the level of gene amplification and/or protein over-expression in ISH and IHC assays respectively. If the invasive tumor shows HER2 over-expression/gene amplification in > 10% of the tumor in a clustered pattern, that carcinoma is considered “HER2-positive” and the patient is a candidate for therapy.
(A) and (C) show intratumoral heterogeneity for HER2 protein over-expression in a clustered pattern and (B) and (D) show the same corresponding area of the tumor from the FISH slide during the low power scan which shows clustered groups of amplified tumor cells adjacent to cells with a normal HER2 genotype. It can be very helpful to used the IHC slide as a guide to target these “hot-spots” with protein over-expression during FISH analysis in cases demonstrating intratumoral-heterogeneity.


Figure 4 legend: HER2 positive breast cancers are aggressive, with a higher rate of recurrence and mortality for those patients who do not receive any adjuvant therapy. These tumors ae more likely to spread early to major visceral site, including brain, lung (A), liver (B), adrenals and ovaries. With the advent of HER2-targeted therapies, progressive visceral disease is significantly diminished. The HER2-alteration is an early and stable genetic change in these tumors, therefore, metastatic HER2-positive breast cancers usually also over-express HER2 at site of distant spread (A&B).
The 2013 HER2 guideline update has placed new emphasis on the importance of performing a repeat biopsy, if clinically possible upon the recurrence of breast cancer for HER2 analysis to help ensure accurate assessment of tumor histology, biology and facilitate appropriate further treatment planning. While for most patients, the HER2 results are similar between the primary tumor and recurrent disease; published reports have shown that the HER2 status may change from negative to positive in 9% to 16% of cases from early to later stage disease, which could potentially dramatically alter subsequent treatment recommendations.
References:
Hicks DG, Tubbs RR. Assessment of the HER2 status in breast cancer by fluorescence in situ hybridization: a technical review with interpretive guidelines. Hum Pathol 2005;36:250-261.
Hicks DG, Kulkarni S. HER2 Breast Cancer: Review of biologic relevance and optimal use of diagnostic tools. Am J Clin Pathol 2008;129:263-273.
Hicks DG, Whitney-Miller C. HER2 testing in gastric and gastroesophageal junction cancers: A new therapeutic target and diagnostic challenge
Appl Immunohistochem Mol Morphol 2011;19:506-508.
Wolff AC, Hammond ME, Hicks DG, et al.; American Society of Clinical Oncology; College of American Pathologists. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J Clin Oncol. 2013 Nov 1;31(31):3997-4013.
URMC First in Region to Offer HER2 FISH Testing for Breast Cancer
"With HER2 testing available right in their back yard, women will be able to more quickly make decisions and be on their path to recovery," said David G. Hicks, M.D., director of Surgical Pathology at the URMC. Read more about HER2 testing.
Our work means a lot to us. That should mean a lot to you and to those you treat.
David Hicks, M.D., is Professor of Pathology and Laboratory Medicine, and Director of Surgical Pathology. He attended medical school at the University of Rochester Medical Center, and completed his residency in pathology at the University of Pennsylvania. He has had prior faculty appointments at the University of Pennsylvania, the Cleveland Clinic and Roswell Park Cancer Institute. His innovative approaches to improving efficiency and quality in surgical pathology have been highlighted in publications, and he has been invited to give lectures sponsored by national pathology organizations. Dr. Hicks is a member of the ASCO/CAP Taskforce that developed the national testing guidelines for ER, PR, and HER2 in Breast Cancer.
View Dr. Hicks' lecture - full screen