Case of the Month: Hematuria and Acute Flank Pain
Case of the Month: Hematuria and Acute Flank Pain
Authors: Dingani Nkosi, MBBS, PhD (PGY-1), Wilrama Lima, MD, DDS (PGY-1), Mark G. Ettel, MD and Hiroshi Miyamoto, MD, PhD
Clinical History
A man in his twenties presented to the emergency department with acute onset of right side flank pain and a history of intermittent gross hematuria for one month. His past medical history was significant for sickle cell trait and presence of a cardiac murmur.
Recent History
Imaging studies showed a heterogeneous enhancing lesion measuring 4.2 x 4.7 x 4.9 cm in the mid right kidney. Enlarged retrocaval and precaval lymph nodes and pulmonary nodules concerning for metastatic disease were also seen. A right radical nephrectomy with retroperitoneal lymph node dissection was performed.
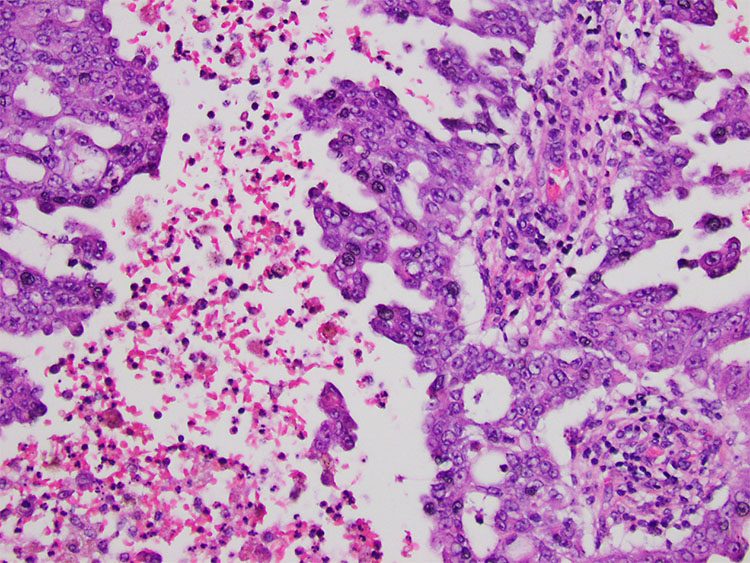
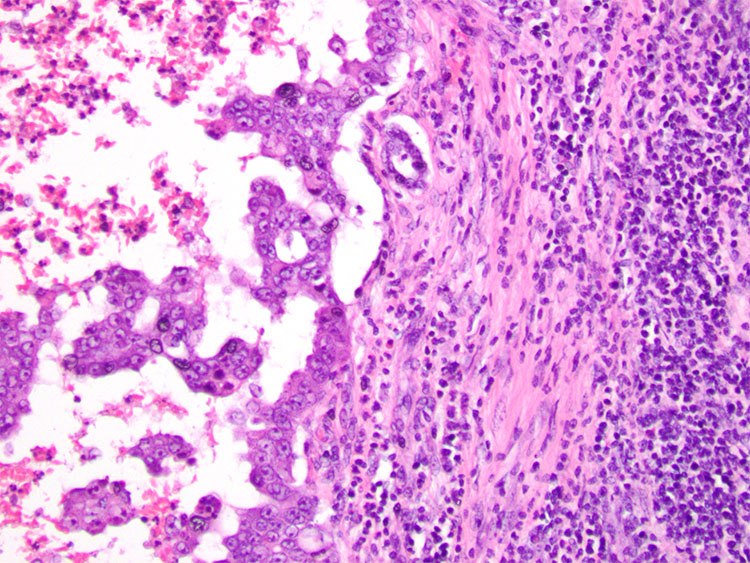
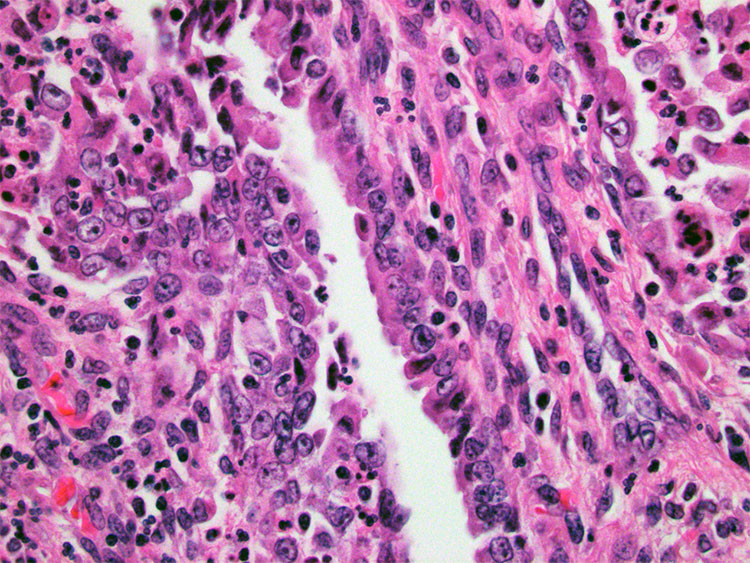
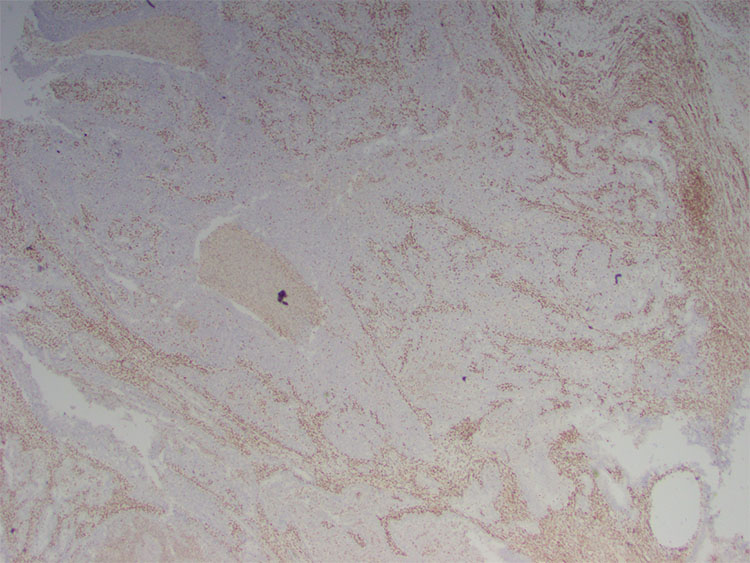
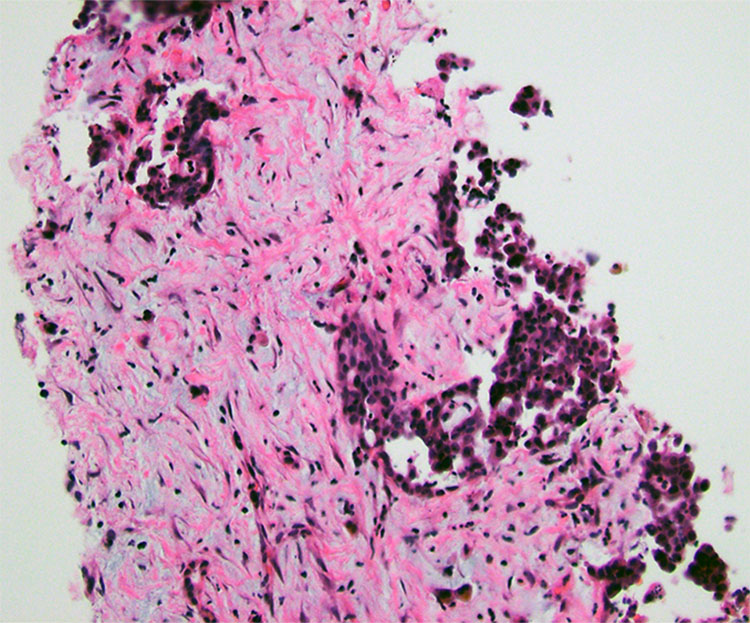
Grossly, the kidney had a 5 x 5 x 3.5 cm white-tan well-circumscribed homogeneous mass with soft, necrotic cut surfaces extending to the kidney capsule (Figure.1). Histologically, the tumor was composed of a mixture of reticular and cribriform growth patterns within a desmoplastic stroma (Figure 2-3). The tumor cells were pleomorphic with eosinophilic cytoplasm and hyperchromatic, enlarged nuclei with prominent nucleoli (Figure 4). Sickled red blood cells were also observed within vessels and the surrounding parenchyma. Immunostaining of the tumor showed positive staining for PAX8 and loss of expression of INI1 (Figure 5). The tumor was noted to invade the pelvicalyceal system with negative surgical margins but had metastasized to two of the twelve regional lymph nodes submitted.
Two months post-surgery, follow-up imaging showed liver lesions. Core needle biopsies of these lesions revealed tumor cells which were morphologically consistent with the primary renal tumor (Figure 6).