Case 7: Chronic Cough
By Nisha Patel, D.O., PGY-3
Clinical history
A 50-year-old African American female with recent travel to the Caribbean presented to the Emergency Department with an 8 week history of cough refractory to antibiotic therapy.
Recent medical history
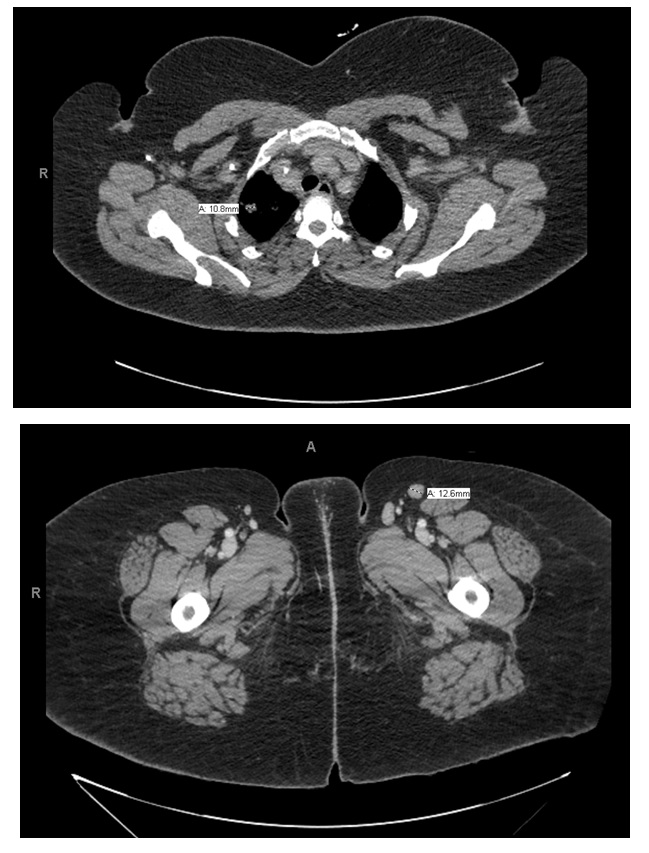
The patient reported a 30 pound weight loss in the last 3 months and recent skin “rash” on back, legs, and arms. CT imaging of the chest and abdomen showed numerous small nodules involving bilateral upper lungs. Cultures of a bronchoalveolar lavage were positive for Pneumocystis jirovecii. Incidentally, bilateral axillary, mesenteric, retroperitoneal, and inguinal lymphadenopathy were also identified on CT (Figure 1).
Imaging
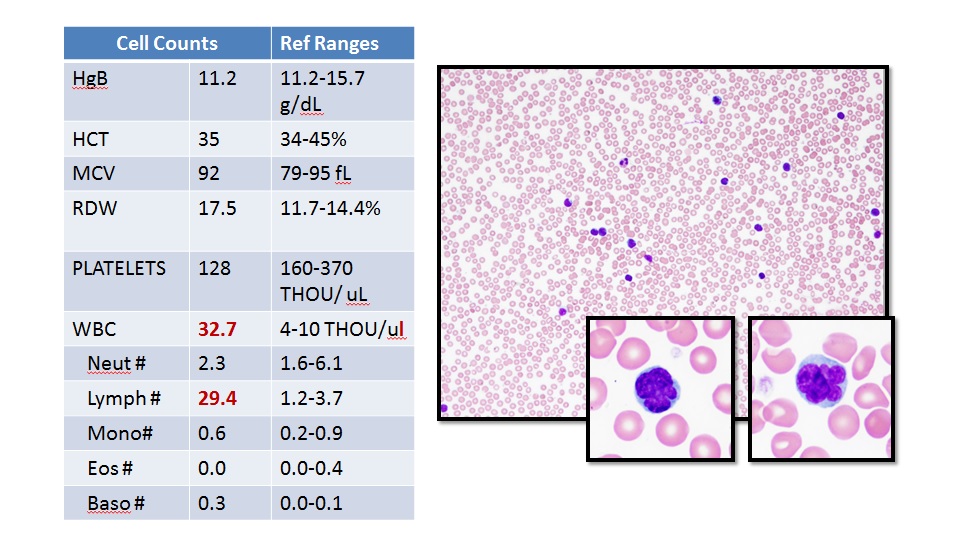
A peripheral blood smear showed marked increase in atypical lymphocytes characterized morphologically by irregular nuclear contours with occasionally clefted and multilobulated nuclei. Flow cytometry revealed that the lymphocyte population was composed essentially of CD3 positive T cells with a CD4/CD8 ratio of 50:1 (Figure 2). This atypical T cell population showed normal expression of CD2, CD3, CD4, CD5, and TCR alpha-beta, with aberrant expression of CD25 (90%), CD30 (5%), and partial loss of CD7 and total loss of CD26. The differential diagnosis included Sezary syndrome, peripheral T cell lymphoma NOS, and HTLV-1 associated adult T cell leukemia/lymphoma.
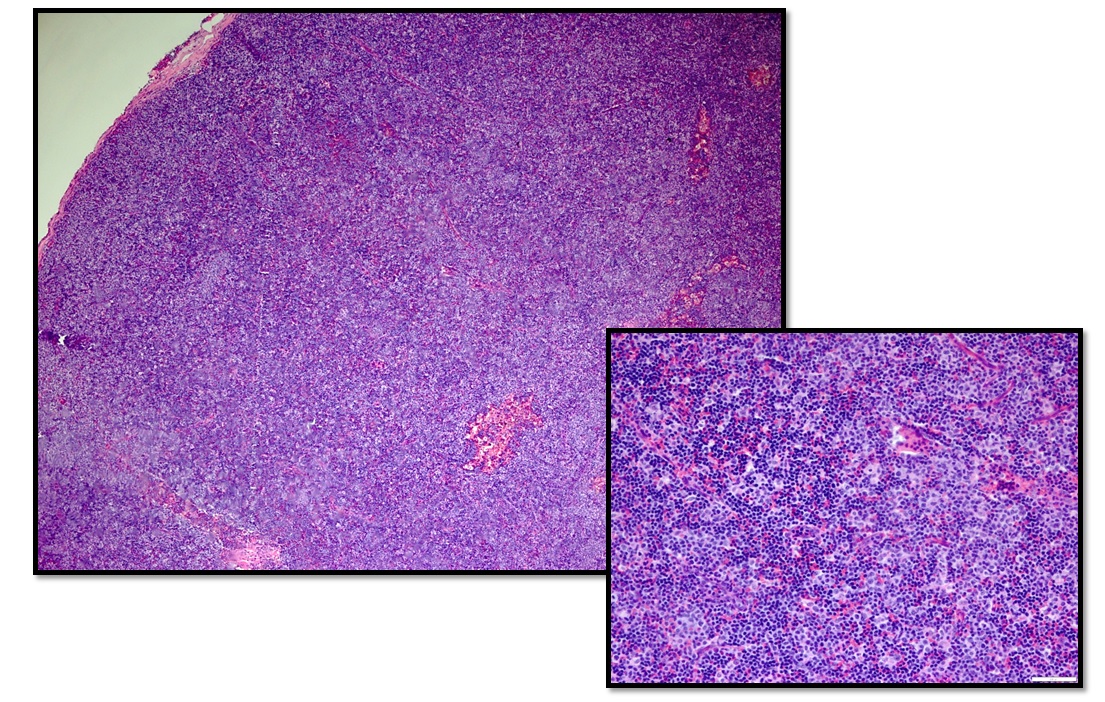
Histologic sections of a left axillary lymph node biopsy revealed diffuse effacement of lymph node architecture by a pleomorphic population of small and large sized atypical lymphocytes. The small sized lymphocytes had irregular nuclear contours, fine chromatin, and prominent nucleoli and larger cells had vesicular chromatin with prominent nucleoli. No necrosis, fibrosis, or inflammatory background was identified. Immunohistochemistry revealed the cells of interest stained positive for CD2, CD3, CD5, and CD25 and were predominantly CD4 positive with scattered CD8 positivity (Figure 3). The atypical population had dim/partial expression of CD7 and variable CD30 positivity but were negative for ALK. CD79a highlighted scattered B cells in residual follicles and was negative in tumor cells.