Meals on Wheels Volunteer Form
Meals on Wheels Volunteer Form
To protect the safety and security of those we serve UR Medicine Home Care will conduct reference and background checks for all potential volunteers. Your signature on the Authorization of Disclosure form authorizes UR Medicine Home Care to conduct a background check to obtain information through criminal record inquiries, public records, and driving record.
If you would like to volunteer for Meals On Wheels, please fill out the form below.
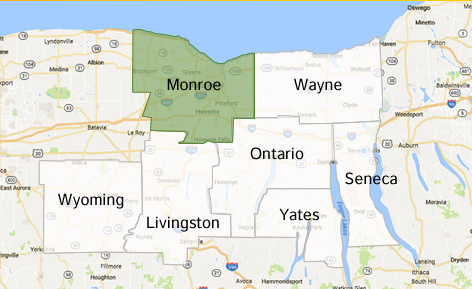
Meals On Wheels Service Area