Middle-Age Female with Presumed Uterine Mass
Middle-Age Female with Presumed Uterine Mass
Alexandria Giese MD, Jordan Payne MD, Roula Katerji MD
Clinical History
A 55-year-old female presented for elective total abdominal hysterectomy with bilateral salpingo-oophorectomy for a presumed large uterine mass with possible involvement of the small bowel. The mass was initially identified during workup for acute symptomatic blood loss anemia secondary to melena.
Past Medical History
The patient’s history was significant for breast carcinoma, hypertension, and hyperlipidemia.
Recent History
During hospitalization for acute symptomatic anemia, CT of the abdomen and pelvis demonstrated a markedly enlarged heterogeneous pelvic mass (Figure 1). Given ongoing melena, the patient underwent outpatient gastroenterology evaluation. Video capsule endoscopy demonstrated a possible small bowel mucosal abnormality without definitive active bleeding or a clear mass lesion. No definitive gastrointestinal source was identified, and surgical management was pursued for a presumed uterine mass with possible bowel involvement.
Surgical Course
At the time of surgery, a large (approximately 15 cm), fungating, friable, hemorrhagic mass was identified within the abdominal cavity. The lesion was separate from the uterus and was found to involve a segment of small bowel, with dense adhesions to the sigmoid colon and pelvic peritoneum. Intraoperative frozen section demonstrated a malignant spindle cell neoplasm with myxoid areas. A segmental small bowel resection was performed. Due to extensive hemorrhage refractory to hemostatic measures, a portion of the tumor was debulked bluntly, while residual disease remained adherent to the pelvic wall.
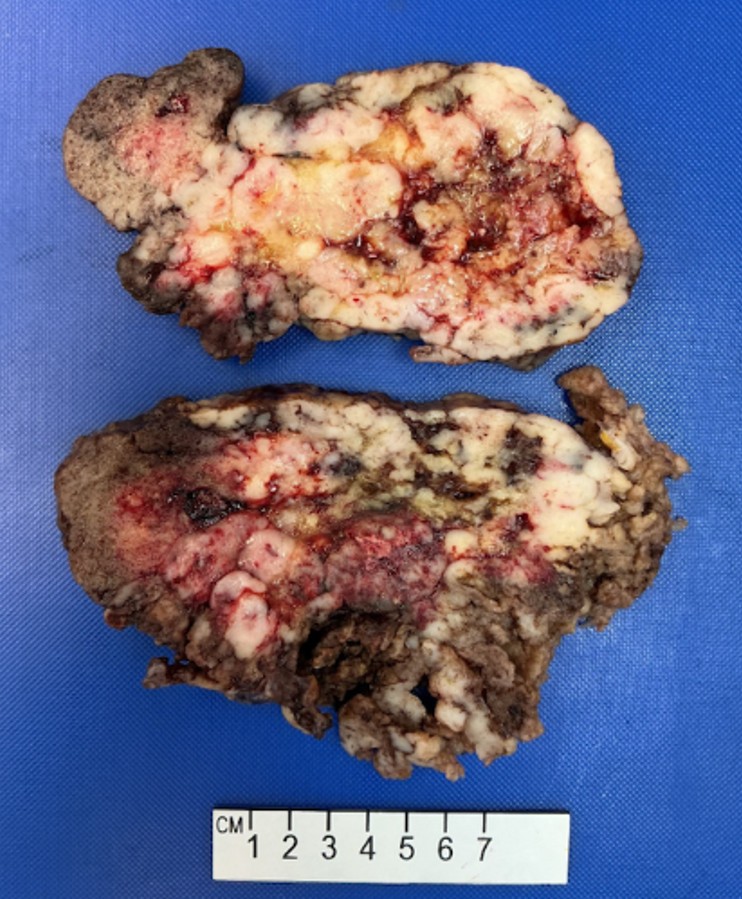
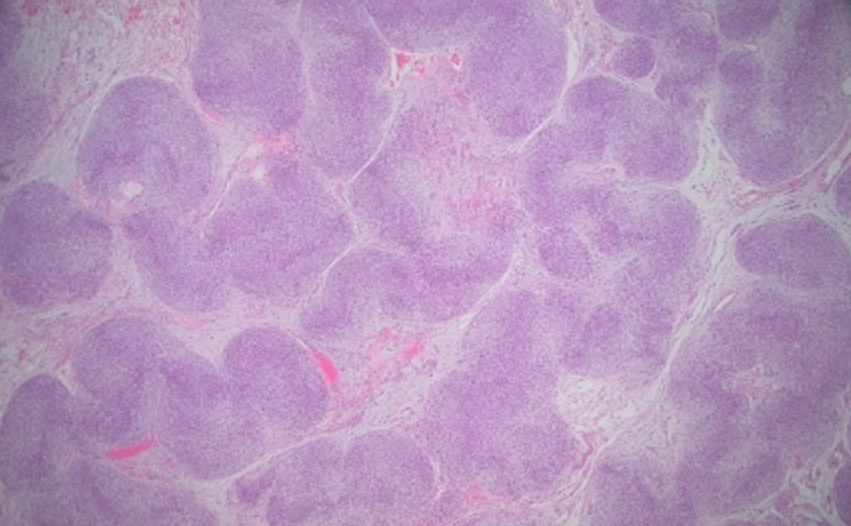
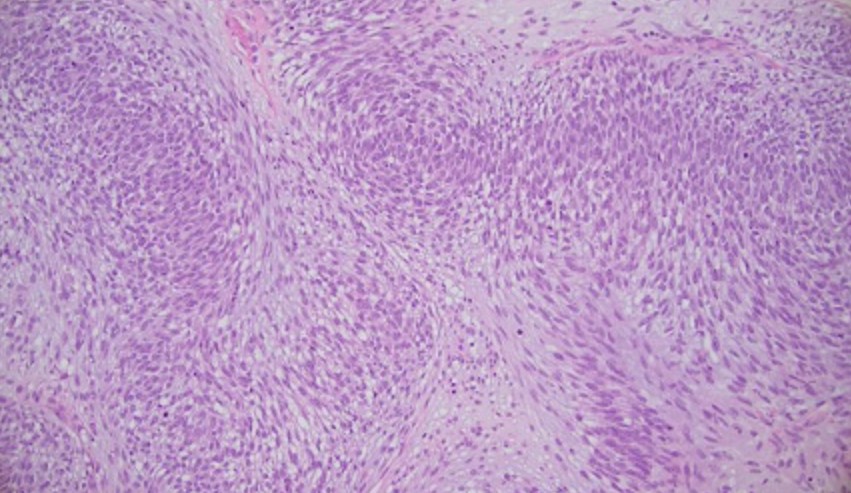
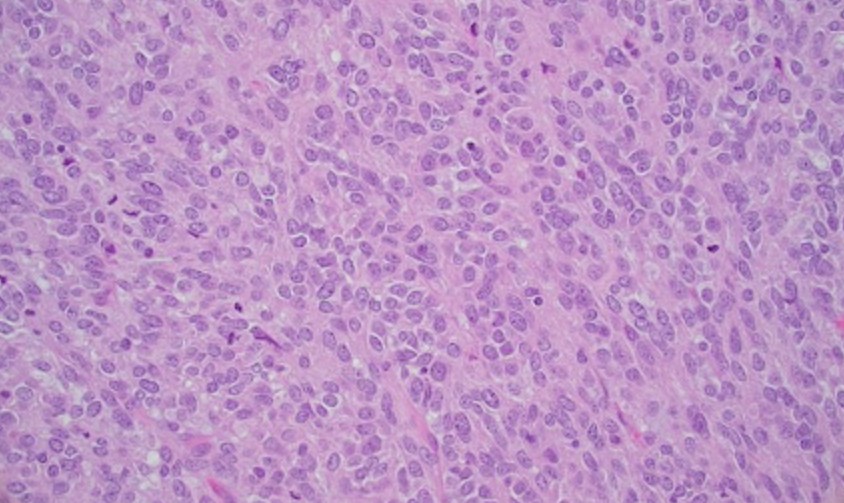
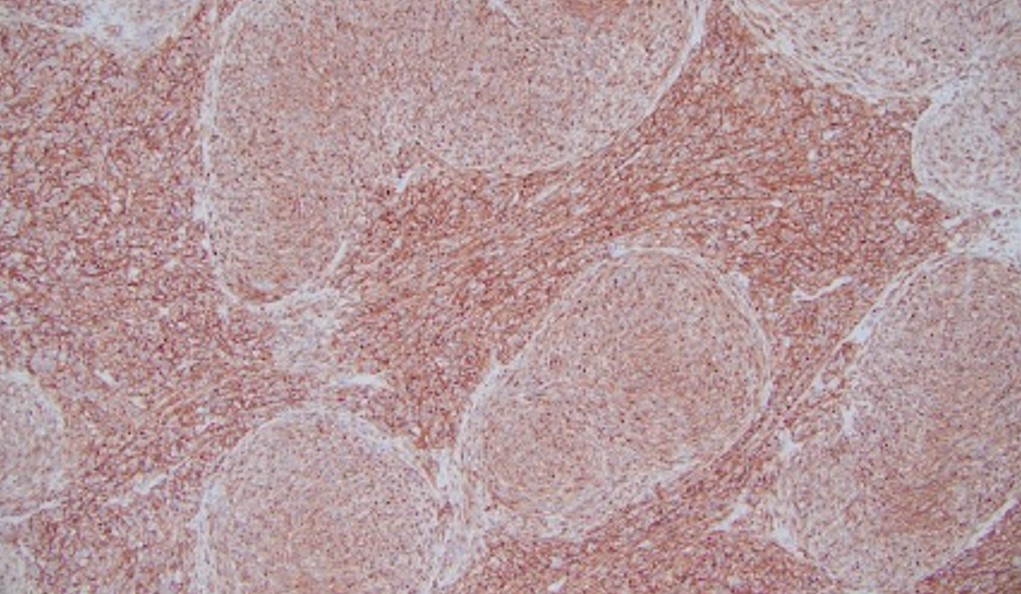
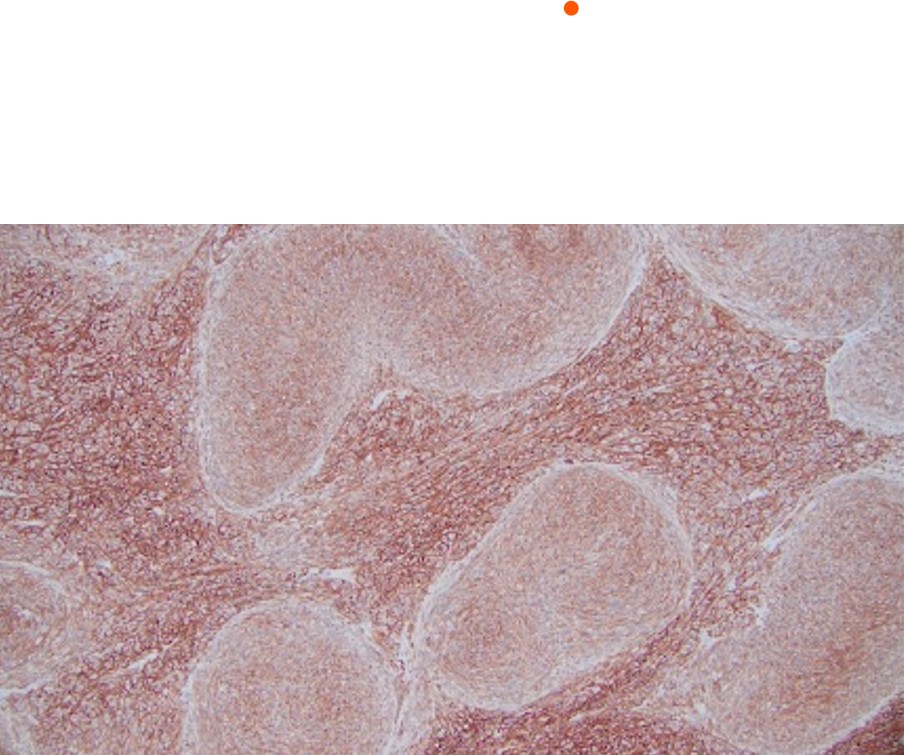
Grossly, the specimen consisted of multiple fragments of rubbery, vaguely lobulated tan-white to brown-gray soft tissue. Cut surfaces were variegated, showing tan-white to pink areas with focal hemorrhage and necrosis (Figure 2). Histologic evaluation revealed a heterogeneous spindle cell and epithelioid neoplasm with areas of necrosis and frequent mitosis (Figure 3-6). Immunohistochemical studies showed strong positivity for KIT (CD117) and DOG1, while negative for ERG, desmin, S100, pancytokeratin, and PAX8.