Case of the Month: Dyspnea
By Deborah Paul, MS4, and Moises Velez, M.D.
Clinical History
A 50-year-old woman with a history of asthma and GERD presents with a one-year history of persistent mild dyspnea treated with inhaled corticosteroid, without much improvement. The patient currently reports chest tightness and discomfort with deep breaths. She recently developed eosinophilia. No history of cough, wheezes, fevers, chills or night sweats. No international travel or recent/remote sick contacts.
Radiology
Chest CT at an outside hospital revealed a RUL infiltrate concerning for an airway lesion versus a mucous plug. A sputum sample was negative for acid-fast bacilli or fungal organisms. Cultures for Legionella and Nocardia were indeterminate because of overgrowth of mold.
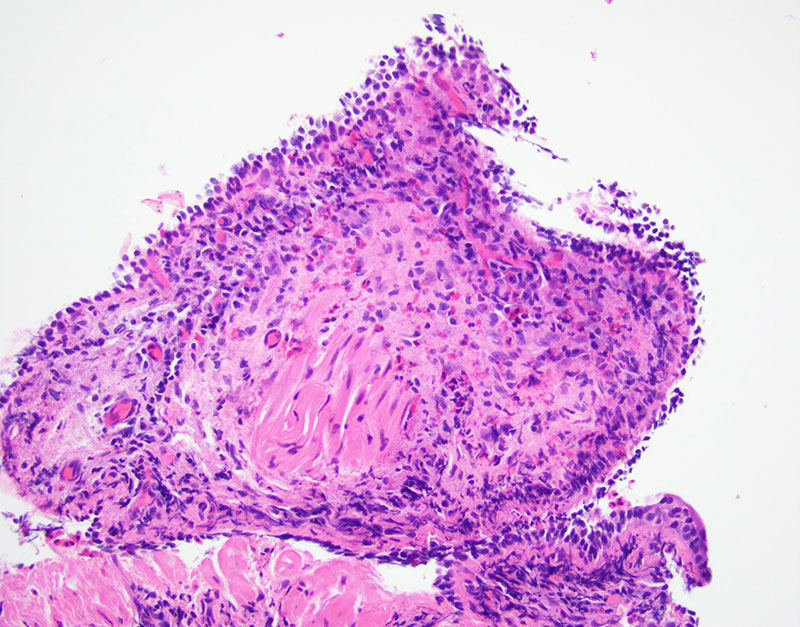
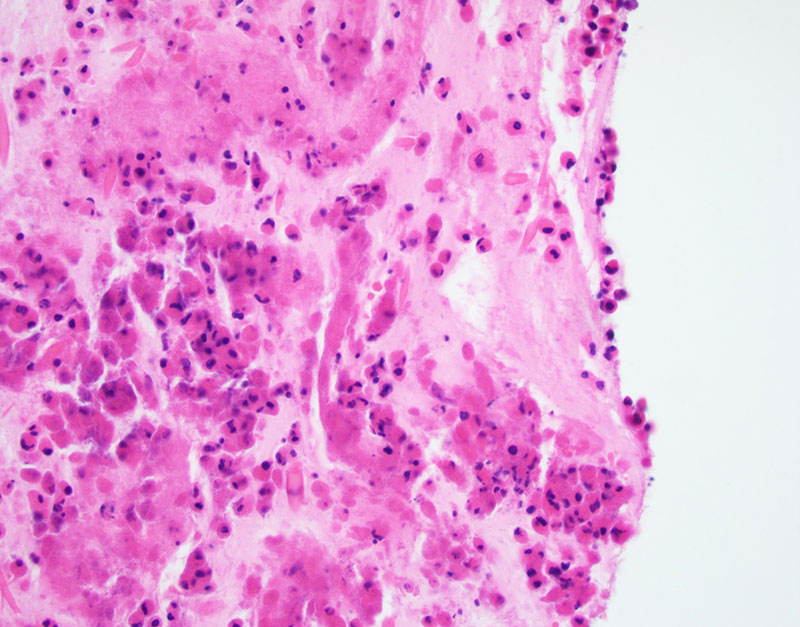
Pathology
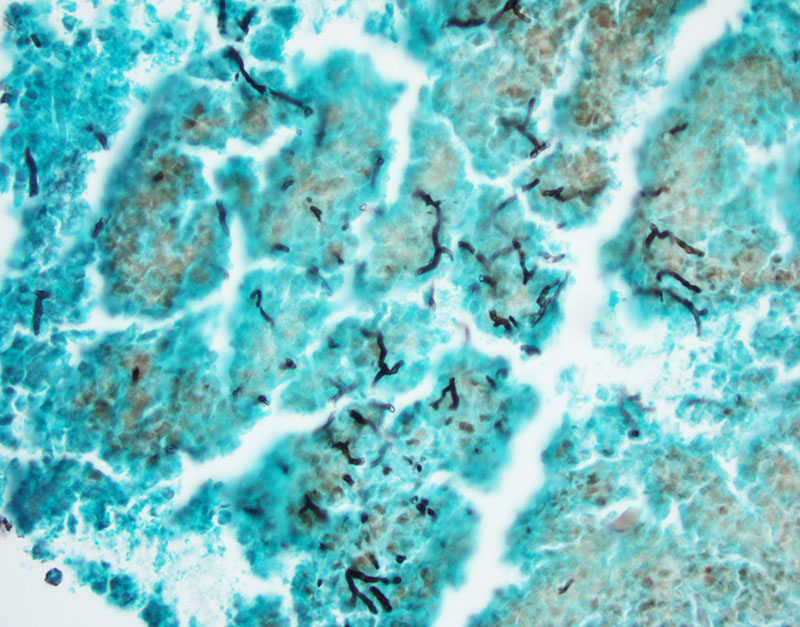
Transbronchial biopsy of the radiographic lesion was done and revealed fragments of bronchial wall and mucoid material with eosinophilic micro-abscesses (Figures 1-2). GMS and PAS stain were performed and highlight fungi with septate hyphae, morphologically suggestive of Aspergillus (Figure 3).