Case of the Month: Shortness of Breath
By Roula Katerji, M.D. (PGY-4), Moises Velez, M.D.
Clinical History
A male, non-smoker, in his fourth decade of life presented with shortness of breath and hoarseness.
Past Medical History
The patient was previously healthy with no clinical problems.
Recent History
At his initial presentation he was diagnosed with anxiety. Six months later he presented to an urgent care clinic with a complaint of fevers, fatigue, cough, sinusitis, night sweating, sinus congestion, and a four week history of nasal drainage. He was started on antibiotics for sinusitis, but symptoms persisted.
Labs noted elevated erythrocyte sedimentation rate, mild anemia, elevated ferritin, and C-reactive protein. Throat and blood cultures were negative. A chest x-ray showed a left lower density consistent with pneumonia. His symptoms did not improve, and the patient was hospitalized for fever and shortness of breath. A chest CT was performed and showed subcarinal lymphadenopathy and a 4.4 cm left lower lobe mass. The radiographic differential included atypical pneumonia or lymphoma. Abdominal CT showed mild bilateral perinephric stranding of uncertain etiology.
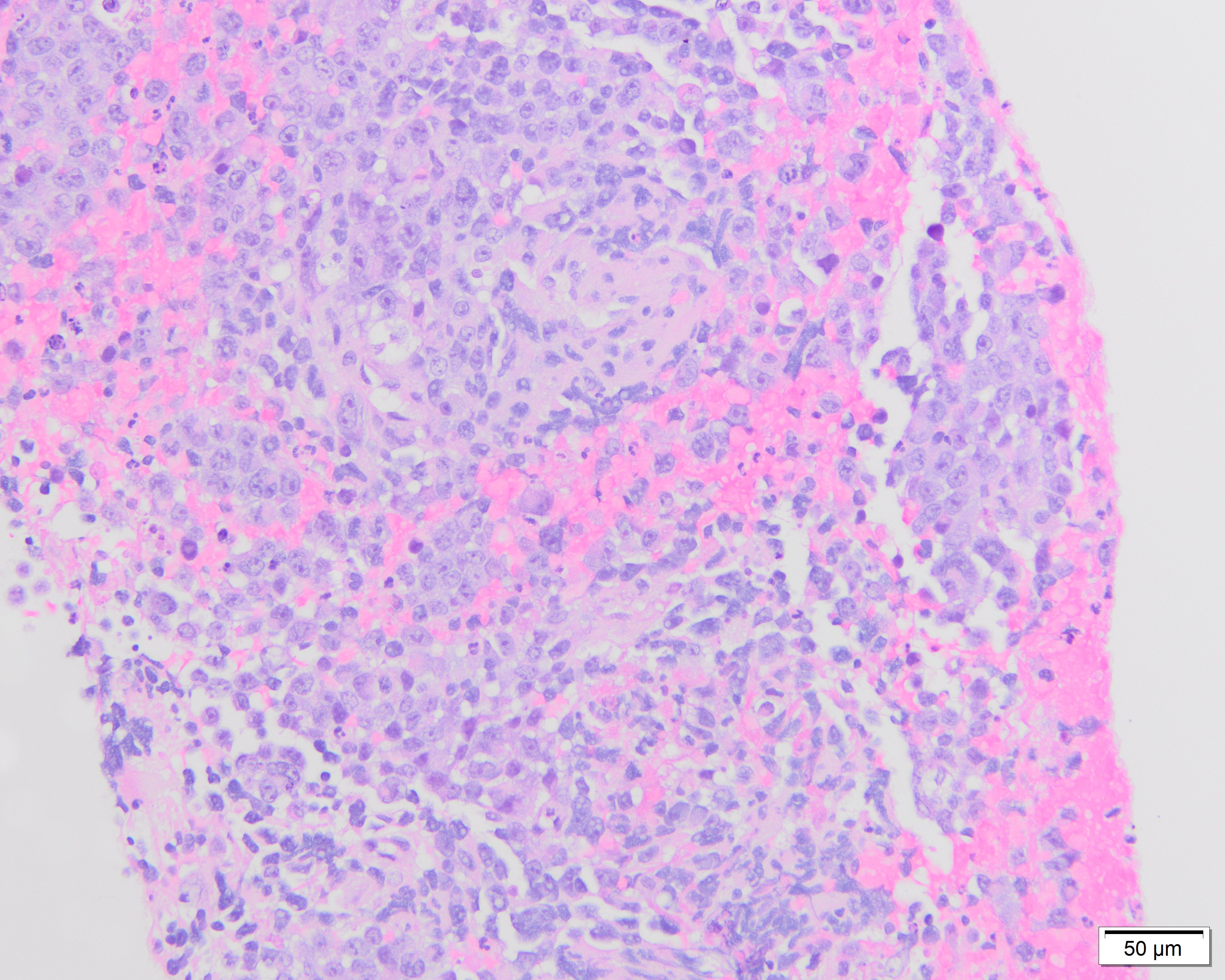
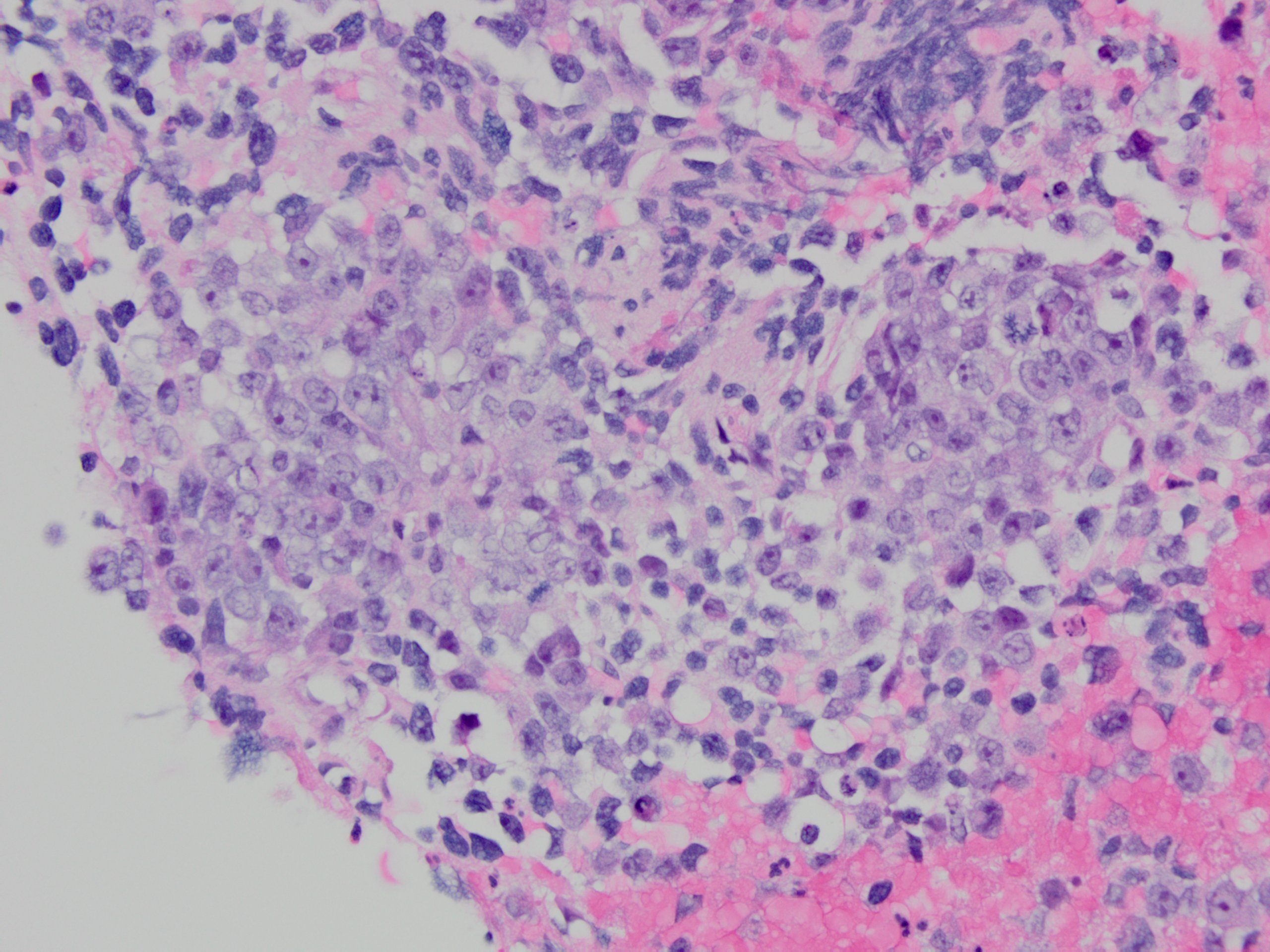
Endobronchial ultrasound (EBUS) biopsy of the station 7/11 left enlarged lymph node was performed and showed undifferentiated epithelioid and pleomorphic round to oval malignant cells.
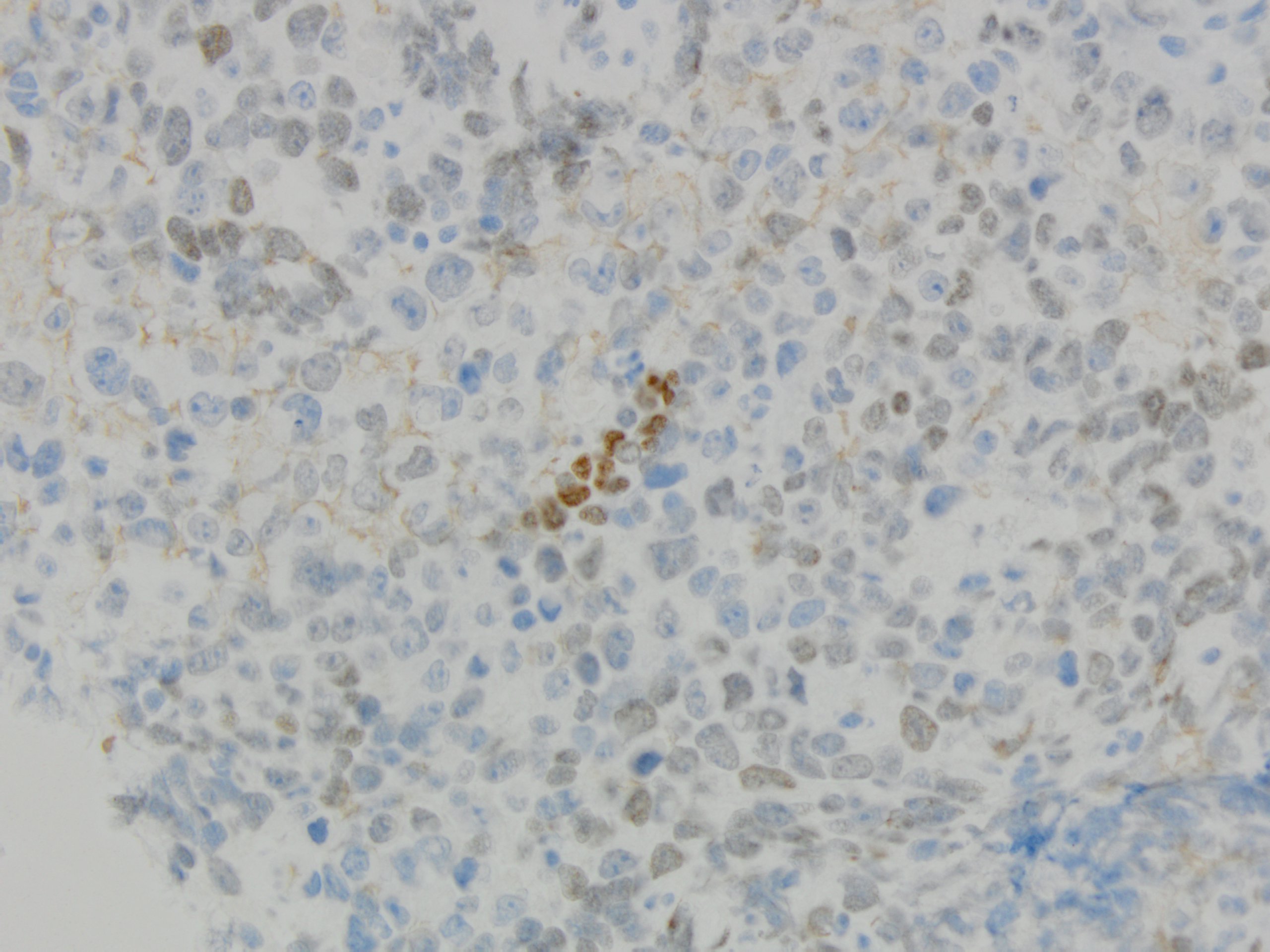
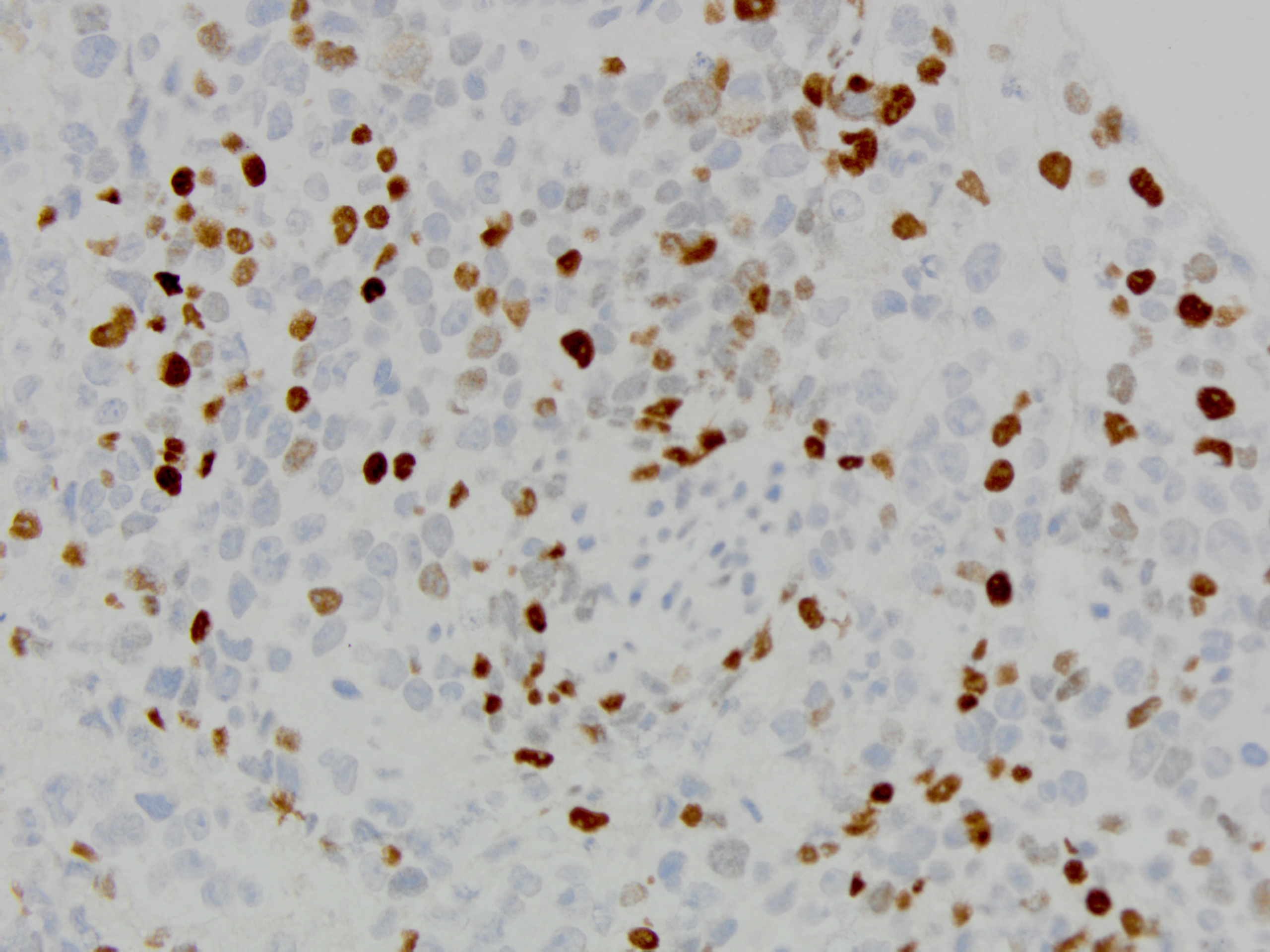
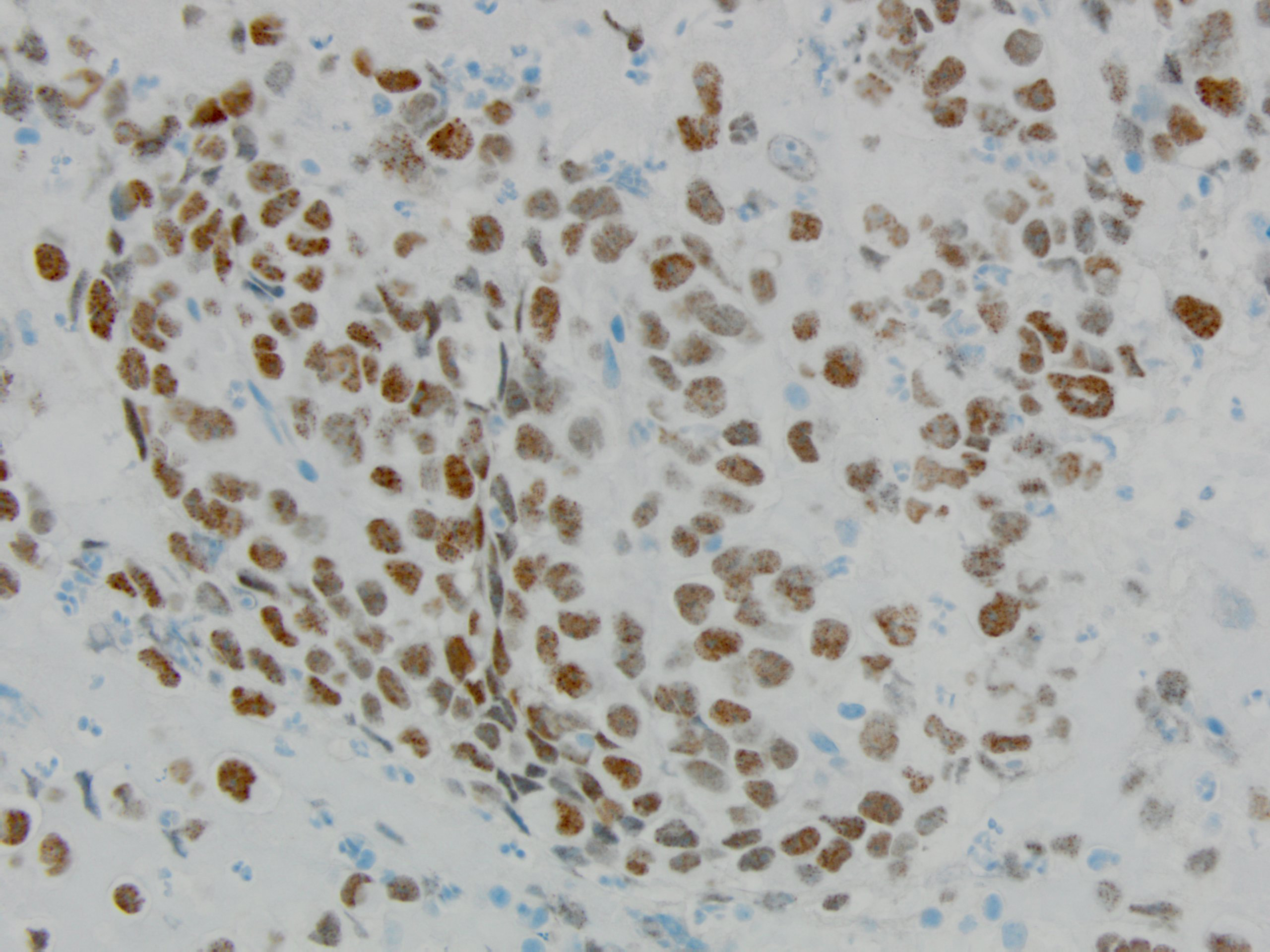
Tumor cells had prominent nucleoli, with areas of necrosis (Figure 1-2). Immunohistochemical stains showed the tumor cells were focally positive for TTF-1 (Figure 3) and p40 (Figure 4) while negative for CD3 and CD20. NUT immunohistochemical stain was positive in tumor cells in a speckled nuclear pattern (Figure 5).
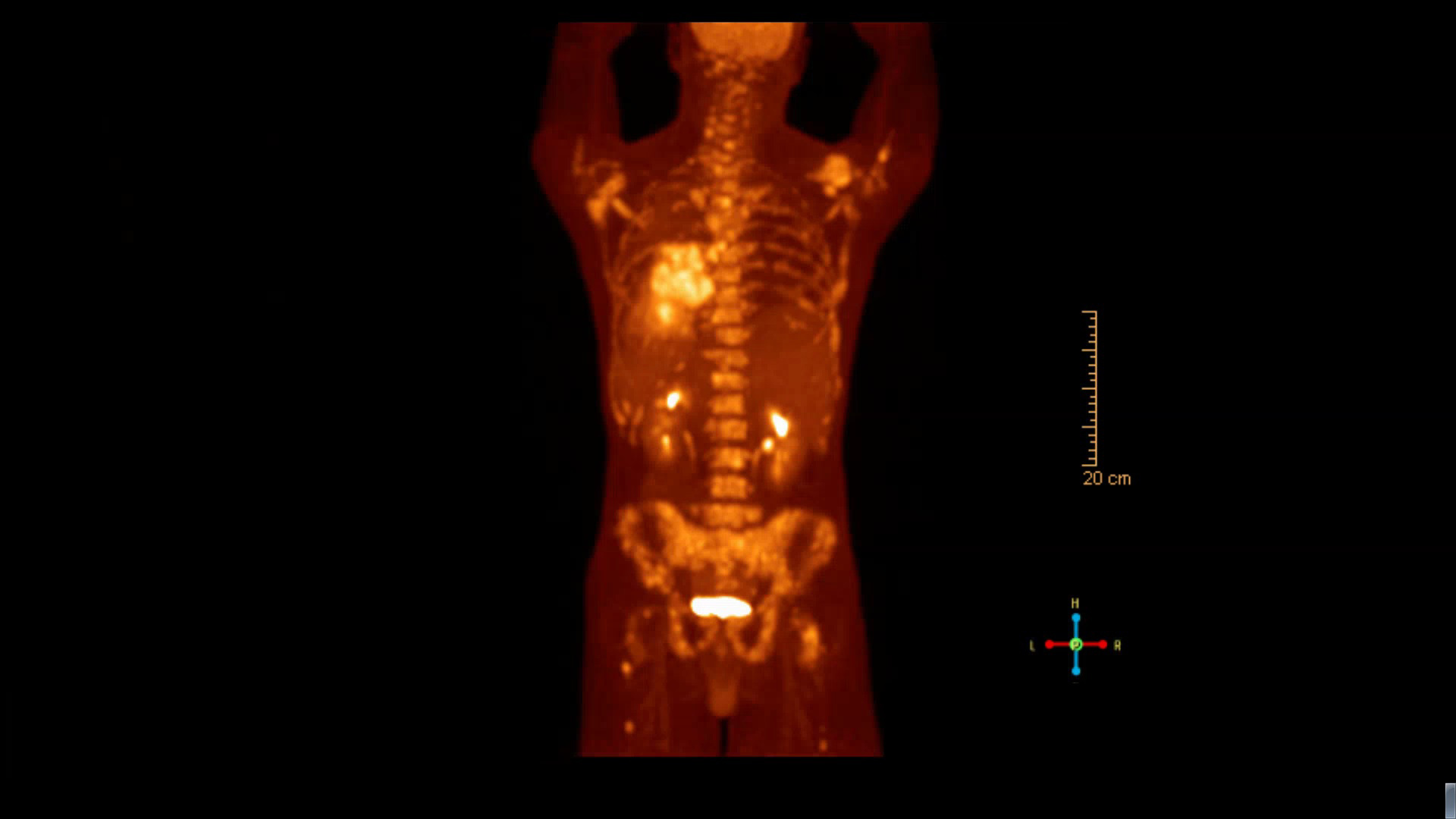
PET scan (Figure 6) was done and showed an intensely hypermetabolic left lower lobe lung mass extending from the pleura to the left hilum with associated small left pleural effusion, consistent with primary lung malignancy. Numerous hypermetabolic left hilar and subcarinal enlarged lymph nodes with frequent hypermetabolic osseous metastases were present throughout the visible axial and appendicular skeleton involving multilevel vertebral bodies, bilateral ribs, bilateral scapulae, sternum, and the pelvic bones.