Ebstein's Anamaloy
Clinical History
A 28 year-old woman was in her 21st week of gestation. The pregnancy was complicated by an abnormal ultrasound that showed cardiac abnormalities. A therapeutic abortion was performed and tissue was sent for cytogenetics.
Gross Examination
The gross examination of the fetus showed a fetal foot length of 3.7 cm, which was consistent with a gestational age of 21 weeks. The heart was focally disrupted with a laceration of the left atrium and complete loss of the pulmonary outflow tract. The heart weight was 2.9 grams. The right side of the heart was notable for an apically displaced insertion of the tricuspid valve. The tricuspid valve also demonstrated an excessively large anterior leaflet. Due to the lower insertion of the tricuspid valve, there was “atrialization” of the superior portion of the right ventricle and dilation of the remaining right ventricle. The left side of the heart was focally disrupted, but otherwise unremarkable.
No other significant pathological abnormalities were identified.
Microscopic Examination
An apically displaced tricuspid valve was confirmed. Within the right ventricle, there was attachment of a short stub of thickened and myxoid tricuspid valve (Figure, below). Additionally, there was another thickened and myxoid valve inserting into the normal position of the annulus at the junction of the right atrium and right ventricle.
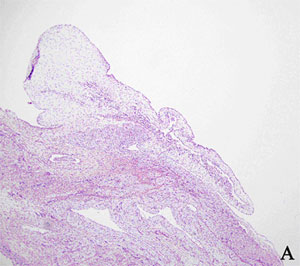
Figure A
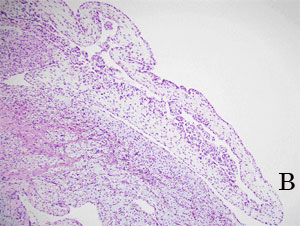
Figure B
Medium (A) and high (B) power images of the thickened and myxoid tricuspid valve leaflet.
Cytogenetics
A normal female karyotype of 46,XX was identified in 20 of 20 cells analyzed.
Discussion
Ebstein's anomaly is a rare congenital malformation that is characterized by abnormalities of the tricuspid valve and the right ventricle. The morphology of the abnormalities is highly variable, but in general, there is downward displacement of the septal and posterior leaflets in a spiral fashion. Thus, those leaflets insert below the true annulus of the tricuspid valve and instead insert into the right ventricular endocardium. The anterior leaflet is attached normally at the annulus of the tricuspid valve and it is typically large, sail-like and containing fenestrations. These changes displace the valvular orifice apically, resulting in an “atrialization” of the proximal right ventricle. In this case, the additionally identified valve inserting into the normal position at the annulus was believed to represent a portion of the septal or posterior leaflet wrapping around in such a spiral fashion.
The leaflets themselves are often dysplastic as well. The septal leaflet is frequently poorly developed and represented only by cauliflower-like remnants along the septum. The posterior leaflet may be rendered immobile as a result of abnormal fusion to the ventricular diaphragmatic wall. The anterior leaflet may also be focally attached to the ventricular wall by short chordae or it may be relatively free and mobile. In addition, fibrous bands may attach the anterior leaflet to the infundibulum. Combined with excess valvular tissue, these findings often result in obstruction of the outflow tract of the right ventricle. In the most severe forms, there may be leaflet malformations resulting in the formation of only an incomplete and rudimentary chamber instead of the right ventricle, as seen in tricuspid atresia (Spitaels 2002).
Other findings within the heart in Ebstein’s anomaly often include a very thin and dilated right atrium, enlargement of the true annulus of the tricuspid valve and an atrial septal defect (ASD), either from a secundum atrial septal defect or a stretched foramen ovale. One review reported that 79 percent of patients had either a persistent or a previously closed patent foramen ovale or an ASD (Attenhofer 2005). The ventricular septum may also bow to the left, resulting in compression of the left ventricle. Associated malformations include pulmonary stenosis and atresia, ventricular septal defect, patent ductus arteriosus and congenital anomalies of the mitral valve. Accessory atrioventricular conduction pathways may also be found within the atrialized right ventricle (Spitaels 2002).
Due to the variety of malformations possible, the pathophysiology of this anomaly is determined by a number of factors, including the morphology of the tricuspid valve itself, the amount of atrial right-to-left shunting, right and left ventricular dysfunction and the presence or absence of tachyarrhymias. In the most benign forms, there are minimal changes and the valve functions normally. Many cases, however, involve some degree of tricuspid regurgitation and stenosis. The increased right atrial pressure and volume enlarges the right atrium, resulting in a right-to-left shunt if a pathway exists. This bypassing of the right ventricle leads to decreased right ventricular stroke volume and the sequelae that stem from that abnormality. Lastly, tachycardia has the deleterious effect of shortening the right ventricular diastolic filling time, leading again to increases in right atrial pressure and decreases in right ventricular stroke volume.
As a result of the stresses that are placed on the cardiovascular system, individuals with Ebstein's anomaly have a shorter life expectancy with only approximately 15% of individuals alive at 60 years (Spitaels 2002). Individuals may present with hemodynamic deterioration, arrhythmias or even sudden death. Infants with Ebstein's anomaly diagnosed in utero have a significantly worse prognosis as compared to others identified later in life. These cases almost always have severe disease with tricuspid regurgitation and significant cardiomegaly. It is believed that one-third of prenatally diagnosed cases will die in utero and only one-tenth will survive the neonatal period (Bianchi 2000).
The etiology of Ebstein's anomaly is unknown. The prevalence is estimated to be 1 in 50,000 to 100,000 individuals with no predilection for gender. Early studies proposed that it might occur with a higher frequency (up to 400 times greater) in infants of mothers who take lithium in early pregnancy. These findings were not supported in later studies, however, and the relationship between first trimester exposure to lithium and Ebstein's anomaly remains unclear (Bianchi 2000).
Ebstein's anomaly is generally considered to be unrelated to karyotypic abnormalities or recognizable syndromes. The majority of cases are sporadic, although familial cases have been reported. It is estimated that the recurrence risk following the birth of an affected child is 1%, while the risk is 3% if there are two siblings already affected (Bianchi 2000).
Alan Sherburne, Student Fellow, 2005-2006
References
-
Attenhofer Jost CH, Connolly HM, O'Leary PW, et al. Left heart lesions in patients with Ebstein anomaly. Mayo Clin Proc 2005; 80:361-8.
-
Bianchi DW, Crombleholme TM, D'Alton ME (editors), Fetology, New York : McGraw-Hill, 2000 pp. 377-81.
-
Spitaels SE. Ebstein's anomaly of the tricuspid valve complexities and strategies. Cardiology Clinics. 20(3):431-9, 2002 Aug.