Placental Mesenchymal Dysplasia (PMD)
Clinical History
A 22-year-old woman presented with the chief complaint of no fetal movement for the past three days. An ultrasound confirmed fetal death in utero and labor was induced the next day. The 29-week stillborn female infant was grossly normal, but the vasculature of the placenta was abnormal.
Gross Examination
The gross examination of the infant revealed several nonspecific findings. Examination of the placenta, though, highlighted several key features. The placenta weighed 397 grams (391 g = Normal for 33-36 weeks) and had a three-vessel umbilical cord. The fetal surface was tan-yellow and had multiple tortuous, distended vessels (Figure 1). Serial sections of the placenta revealed multiple tan-white vesicles, ranging from 0.6 to 5.0 cm, filled with thick, serous fluid (Figure 2, 3). On the maternal surface, there was a thick, tan-white infarct occupying 60% of the surface (Figure 4).
Click an image to view larger format.

Figure 1

Figure 2

Figure 3

Figure 4
Microscopic Examination
There was microscopic identification of convoluted myxoid vessels in the chorionic plate and hydropic stem vessels (Figure 5). In addition, there were edematous terminal villi (Figure 6). Most importantly, no trophoblast hyperplasia or trophoblastic inclusions were noted when compared to partial moles (Figure 7). Overall, these gross and microscopic findings are consistent with placental mesenchymal dysplasia.
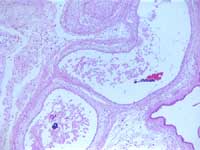
Figure 5: Dilated stem vessels
Figure 6: Edematous villi
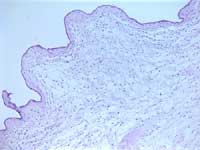
Figure 7: PMD edematous villus with simple trophoblast layer
Cytogenetics
Placenta and fetal skin were sent for karyotype analysis and the results were inconclusive. There was no metaphase spreads available for analysis after 14 days of cultivation. Subsequent analysis with FISH revealed an XX sex chromosome composition with no numerical aberrations for chromosomes 13, 18, and 21. The diploid karyotype (versus triploid seen in partial hydatidiform mole) further supports the diagnosis of placental mesenchymal dysplasia.
Discussion
Placental mesenchymal dysplasia (PMD), also known as pseudo-partial mole, is a rare disorder with approximately 51 cases reported worldwide. The true incidence of the disorder is unknown. The disorder is characterized by placentomegaly with markedly hydropic stem villi that resemble a partial mole, but there is no trophoblastic proliferation. In addition, the karyotype is usually normal and it is thought to have a female predominance (46 XX). PMD has been found to be associated with Beckwith-Wiedemann syndrome.
It is important to distinguish PMD from partial hydatidiform moles. Various fetal complications have been reported in infants associated with PMD. These include intrauterine growth restriction, fetal anemia, thrombocytopenia, prematurity and intrauterine fetal death. Maternal complications associated with PMD are comparatively rare. Partial hydatidiform moles require clinical follow-up to document decreasing beta-hCG levels since there is a small risk for persistent gestational trophoblastic disease.
Gross and histological findings distinguish PMD from partial hydatidiform moles. Grossly, as seen in this case of PMD, there is aneurysmal and varicose dilatation of chorionic vessels. In addition, there are large areas of cystic villous changes. By histology, there is excessive trophoblast proliferation and trophoblastic inclusions in partial hydatidiform moles. These findings are not present in PMD. Histologic findings in PMD include areas composed of enlarged stem villi with cistern-like formation intermixed with normal placental tissue. Chorioangiomatoid changes may also be present.
Tobechi Ebede, Student Fellow 2004
References
-
Arizawa M, et al. Suspected involvement of the X chromosome in placental mesenchymal dysplasia. Congenital Anomalies 2002; 42:309-317.
-
Chan YF, et al. Placental mesenchymal dysplasia: A report of four cases with differentiation from partial hydatidiform mole. Australian and New Zealand Journal of Obstetrics and Gynecology 2003; 43: 475-479.
-
Jauniaux E, et al. Perinatal Features Associated with Placental Mesenchymal Dysplasia. Placenta 1997; 18: 701-706.
-
Paradinas FJ, et al. Pseudo-partial moles: placental stem vessel hydrops and the association with Beckwith-Wiedemann syndrome and complete moles. Histopathology 2001; 39: 447-454.