Case of the Month: Ovarian Cyst
By Shana Straub, MD (PGY-4)
Clinical history
A 16-year-old female with a history of ovarian cysts and increasing LLQ pain. She had been on progestogen-only pills for at least 2 years prior to presentation. An ultrasound showed a complex cyst on the right ovary. This was followed-up with monthly ultrasounds, with each subsequent scan showing growth of the cyst. By 3 months of follow-up, the cyst was 5.5 x 4.7cm. The patient was scheduled for laparoscopy and ovarian cystectomy.
Past medical history
Patient has history of migraine headaches with aura, depression/anxiety. No significant prior surgical history.
Recent history
During the initial laparoscopy, the right ovarian cyst was noted to be filled with yellow-fluid and an adipose-like material. The cyst ruptured in the OR during blunt dissection, and was sent to pathology as an aggregate of pink-yellow fibromembranous tissue fragments.
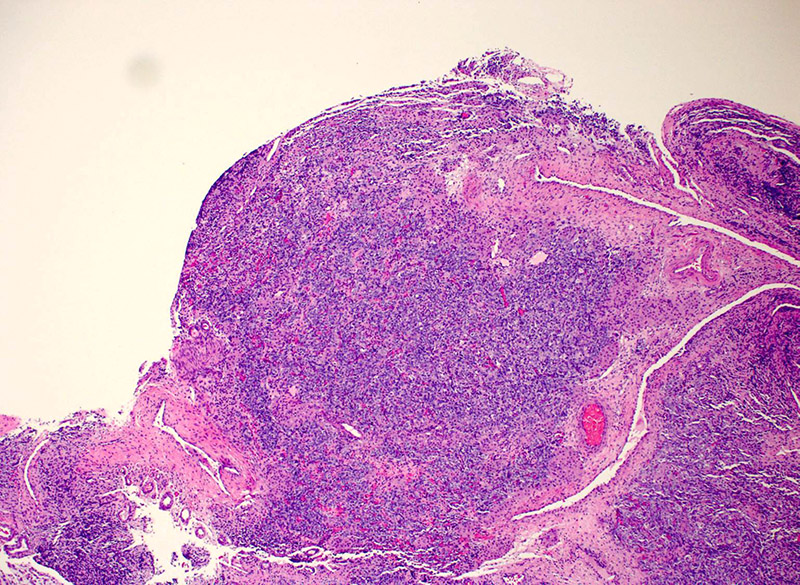
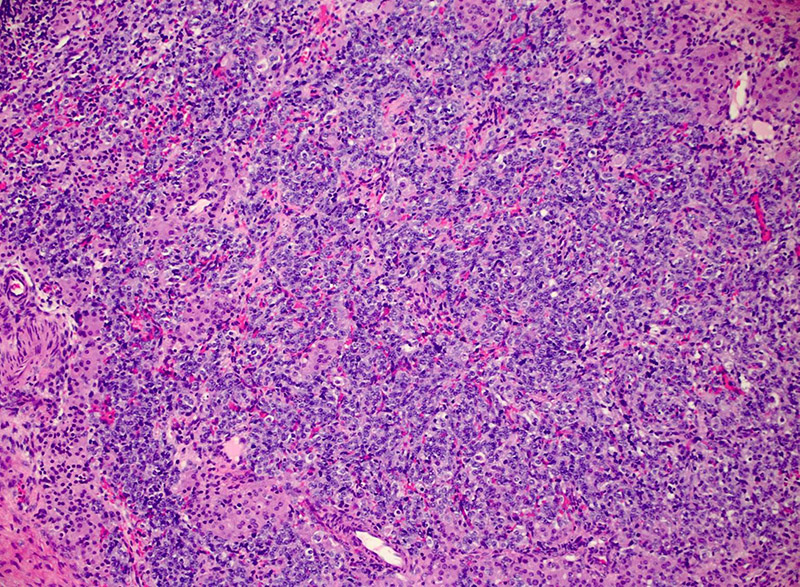
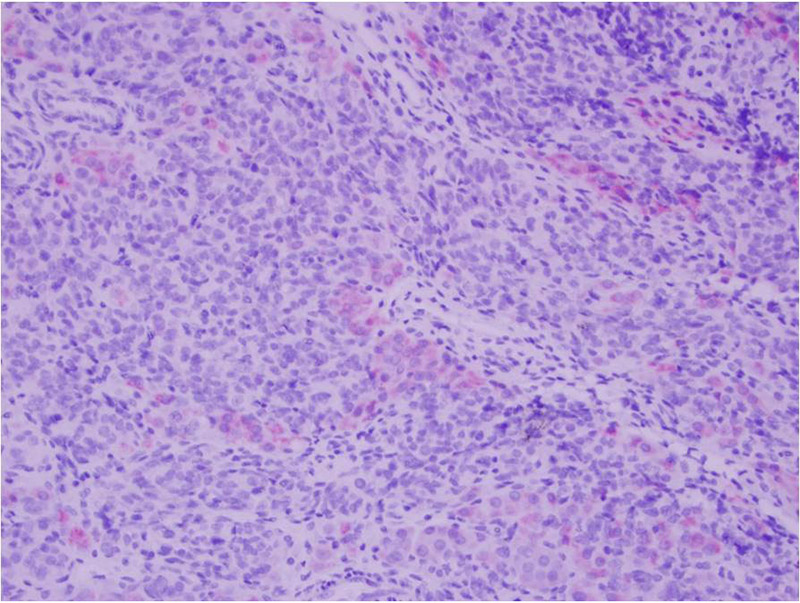
On microscopic examination, the specimen showed a lobulated hypercellular tumor consisting of 2 cell populations. The predominant population was columnar basophilic cells arranged in irregular cords and nests with vague tubule formation. There were also small infrequent nests and clusters of plump eosinophilic to pale cells with round nuclei containing prominent nucleoli (Figures 1 and 2).
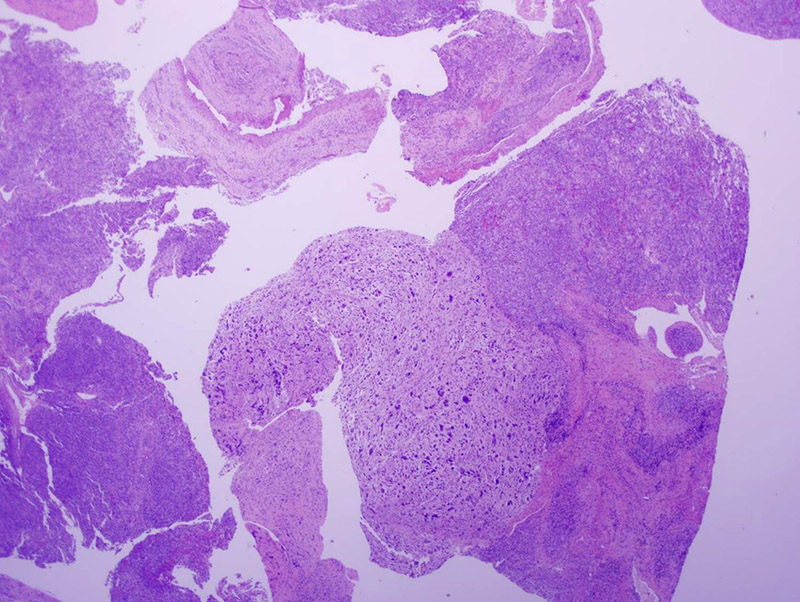
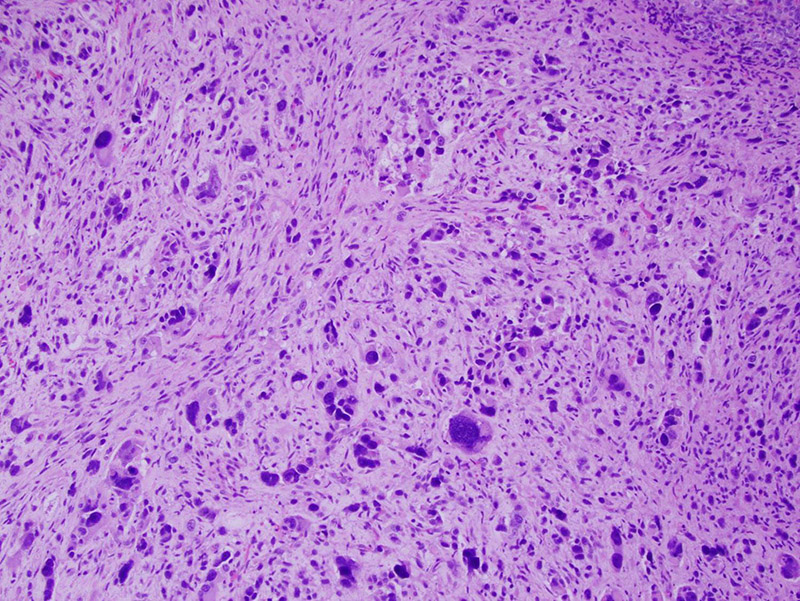
Scattered throughout the specimen were areas with heterologous sarcomatous elements, showing a spindle cell population with marked pleomorphism and hyperchromasia (Figures 3 and 4).
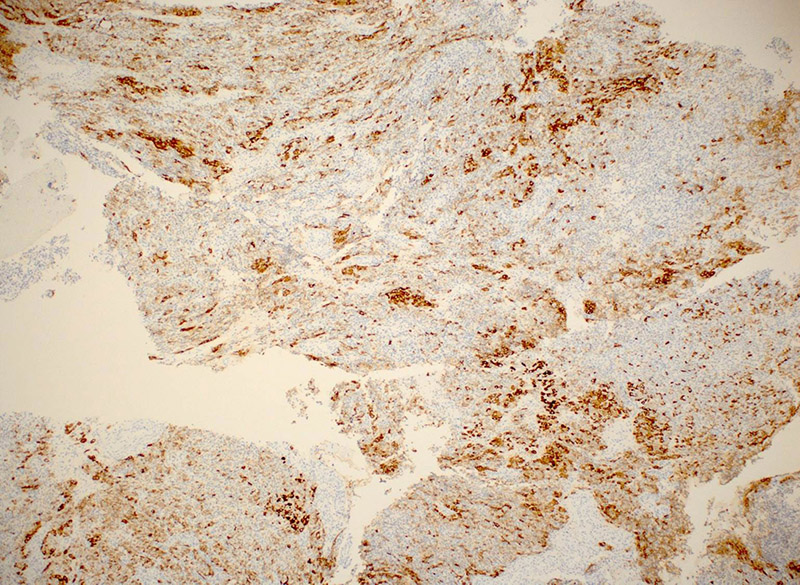
Immunohistochemical (IHC) stains were performed. Both cell populations were positive for inhibin (Figure 5), though more strongly so in the eosinophilic cells, which were also positive for Melan-A (Figure 6). The tumor cells were also positive for pancytokeratin and vimentin, and were negative for EMA.