Case of the Month: Dysphagia
By Jennifer Findeis-Hosey, MD
Clinical History
An 82-year-old female with a reported history of GERD. The patient has a reported history of recent nausea, vomiting, and occasional difficulty with swallowing.
Past Medical History
The patient had a repeat partial fundoplication secondary to recurrent hiatal hernia in the preceding year. Past medical history includes GERD, hiatal hernia, heartburn, hypertension, TIA, arthritis, coronary artery disease and myocardial infarction. Current medication list includes aspirin, pantoprazole, atorvastatin, metoprolol, and clopidogrel.
Recent History
The patient underwent an esophagogastroduodenoscopy (EGD) with biopsy. The proximal esophagus was unremarkable, while there were white plaques in the mid esophagus and a circumferential white coating of the distal esophagus. The endoscopic differential included Candida esophagitis or exudative esophagitis. The stomach and duodenum were unremarkable endoscopically and histologically.
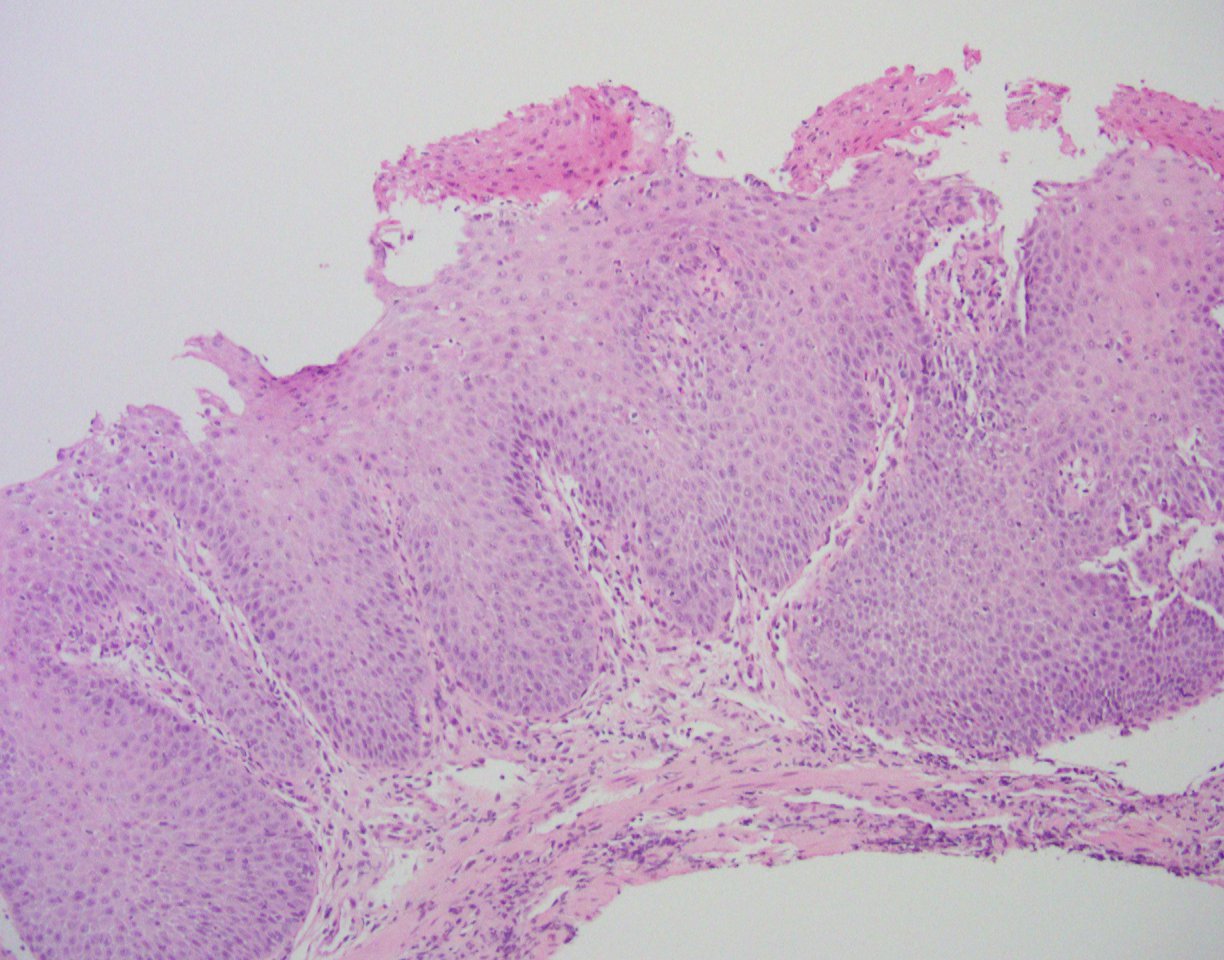
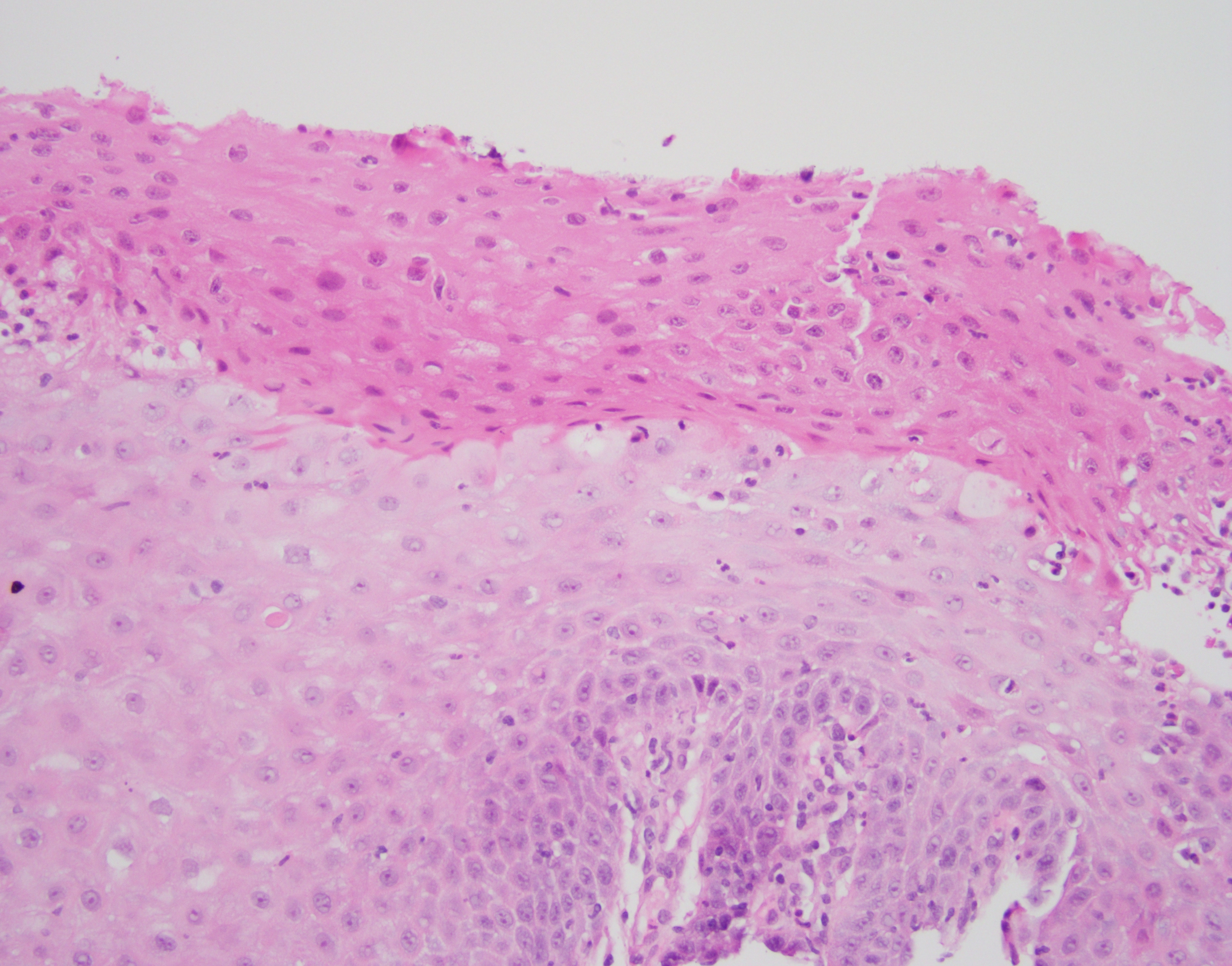
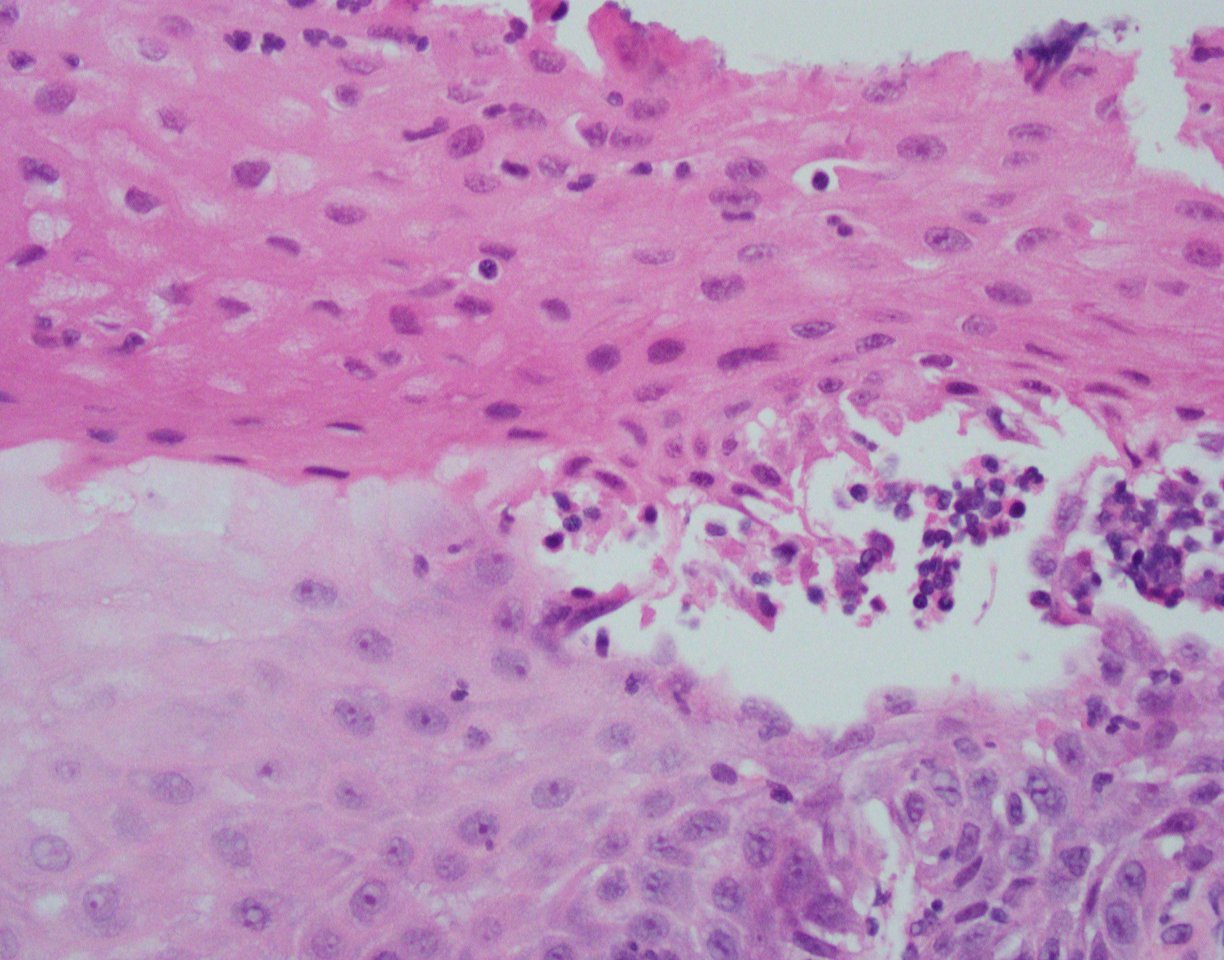
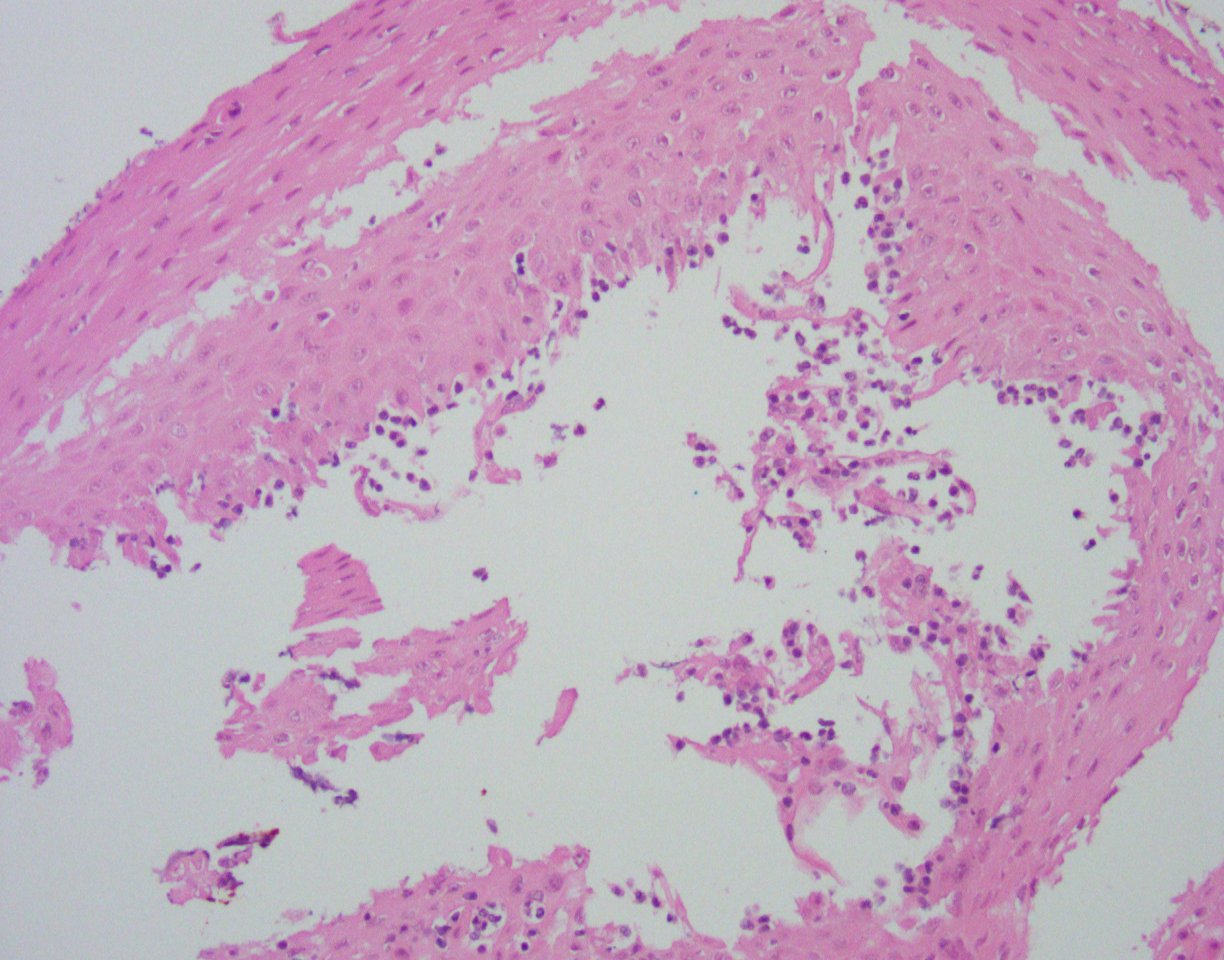
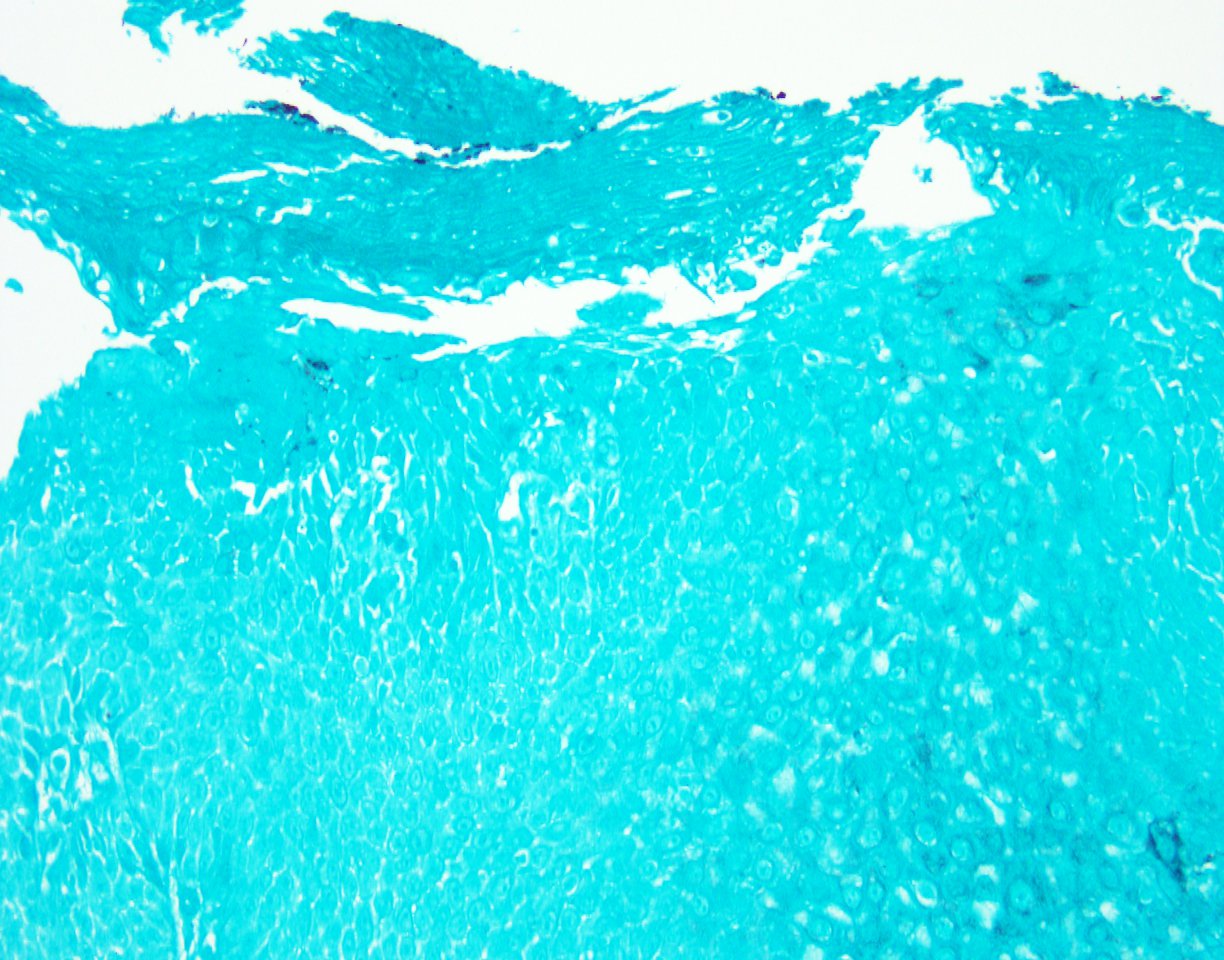
Histologically, the esophageal mucosa demonstrates hypertrophied squamous epithelium with a superficial zone of eosinophilic epithelium (Figures 1, 2). The superficial epithelium exhibits necrosis with faded or ‘ghost-like’ nuclei (Figure 2). A band of neutrophilic inflammation can be seen in some areas separating the two epithelial layers (Figure 3). Some of the tissue fragments in this biopsy specimen consist solely of the superficial necrotic material and neutrophilic junctional layer (Figure 4). GMS stain is negative for fungal organisms (Figure 5).