Case of the Month: Pleural Effusion
By Phoenix Bell, MD, MS, and Moises Velez, MD
Clinical History
A 78-year-old female presented with a 1.5-month history of fatigue, decreased appetite, nausea, 5lb weight loss, and night sweats. She denied shortness of breath, chest pain, abdominal pain, fever, and chills. Two months prior to this presentation, she was diagnosed with shingles and completed a course of acyclovir and gabapentin. Upon physical exam, decreased breath sounds and dullness to percussion were noted in the right lower lobe.
Past Medical History
The patient has a past medical history of a cancerous colon polyp removed in 2006, hypertension, hyperlipidemia, lumbar spinal stenosis, and left parotid gland pleomorphic adenoma s/p left parotidectomy in 2016. Her family history includes a brother who passed away from brain cancer and a father who passed away from lung cancer. She has never smoked, drinks 2 alcoholic beverages a week, and has never used illicit drugs. She has no occupational exposures.
Recent History
The patient was sent for a CXR, which revealed a moderate right-sided pleural effusion. Follow-up chest CT with contrast demonstrated a large right-sided pleural effusion. There were pleural nodules and larger diaphragmatic nodules in the remaining aerated right hemithorax. Lobulated subcarinal adenopathy measuring up to 3.4 x 2.8cm was identified. A small left lung nodule and a pleural nodule were noted involving the lingula and abutting the pericardium.
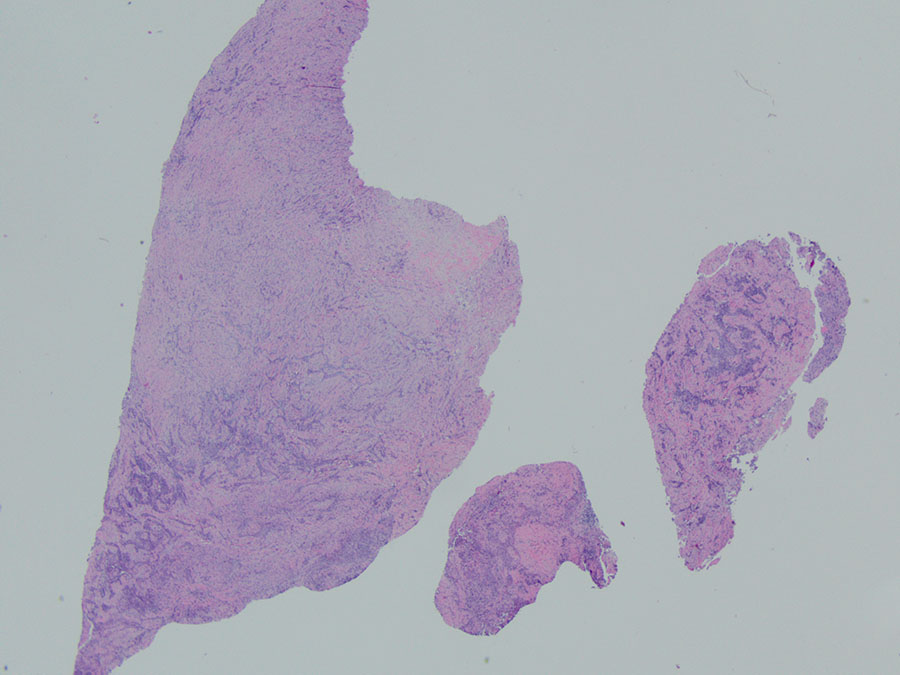
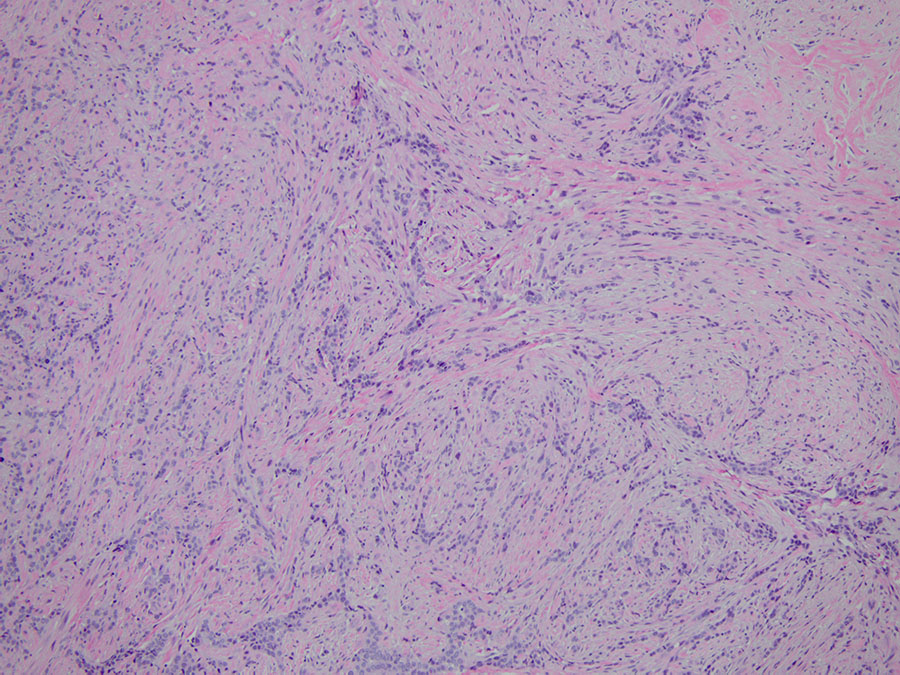
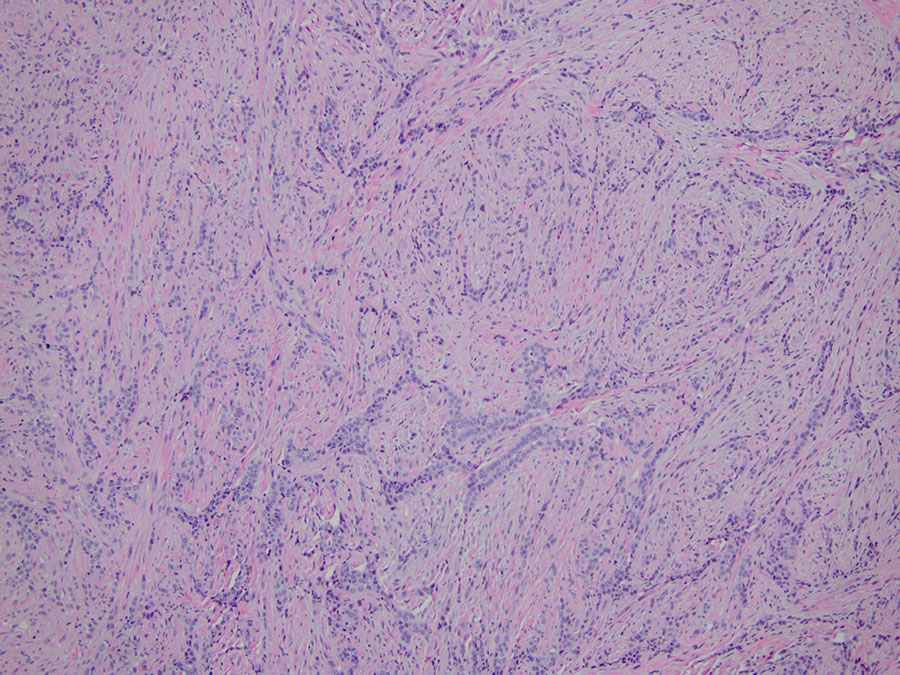
A right video-assisted thoracoscopy was performed and two chest wall biopsies were taken. Fragments of tan-white soft tissue were received, measuring up to 1.8cm in aggregate. Upon histologic evaluation, low-power magnification (2X) revealed a neoplasm with biphasic morphology (Figure 1). Sheets of epithelioid cells were noted within a background of dense fibrosis. Cytologically, the tumor cells appeared monotonous, showing round nuclei with prominent nucleoli. Mitotic figures were inconspicuous (Figure 2). Atypical spindled to ovoid tumor cells were noted in streaming fascicles within dense hyalinized fibrous stroma (Figure 3). The interface of these two patterns is seen in Figure 4. Focal invasion into chest wall fat is noted (Figure 5). The diagnosis was confirmed with positive stains including D2-40, WT-1, calretinin, and pancytokeratin (Figures 6-9). The tumor cells were negative for TTF-1, p40, CEA and CD15.