Case of the Month: TMJ Destructive Lesion
By Catherine Sheils, MD
Clinical History
A 68-year-old female presents with increased swelling in the left temple with associated mild tenderness. On physical exam the external auditory canal appears to have been encroached and inflammation was noted in the zygomatic arch region.
Past Medical History
The patient’s history is significant for a left temporal craniectomy with temporomandibular joint (TMJ) remodeling for treatment of biopsy-proven pseudogout tophus 6 years earlier.
Recent History
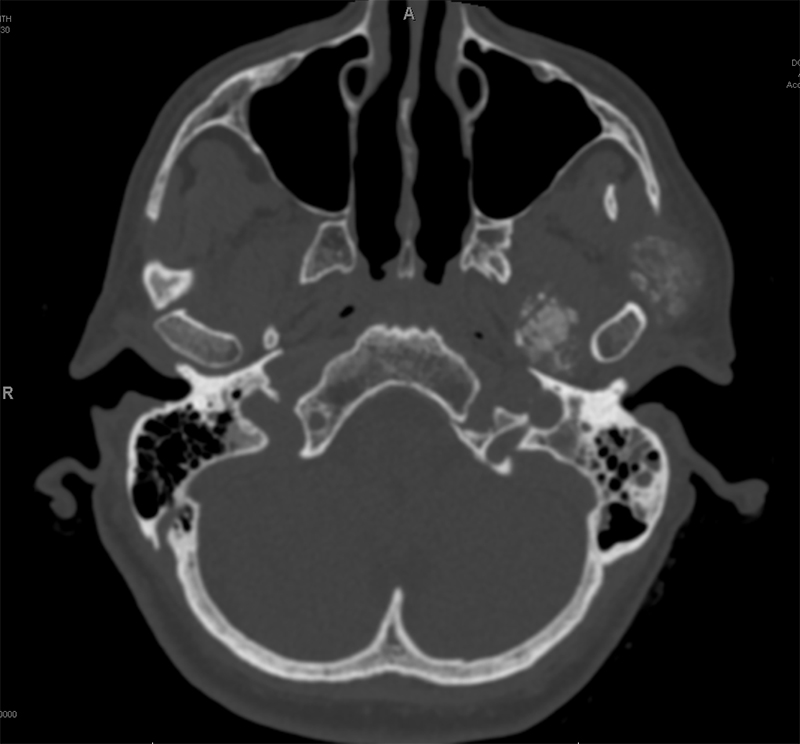
CT scan demonstrates interval increase in tophi size and localized destruction around the left TMJ (Figure 1). The lesion extends into the left middle ear and auditory canal, with increased destruction of the left zygomatic arch. MRI reveals heterogenous, enhancing mass-like extracranial lesions at the left sided skull base surrounding the left TMJ, noted to be larger in size and number compared to MRI from 6 years earlier (Figure 2). Erosive osseous changes and osseous re-modeling at the left skull base were also noted. The findings were interpreted as compatible with previously biopsy-proven pseudogout with evidence of recurrent disease.
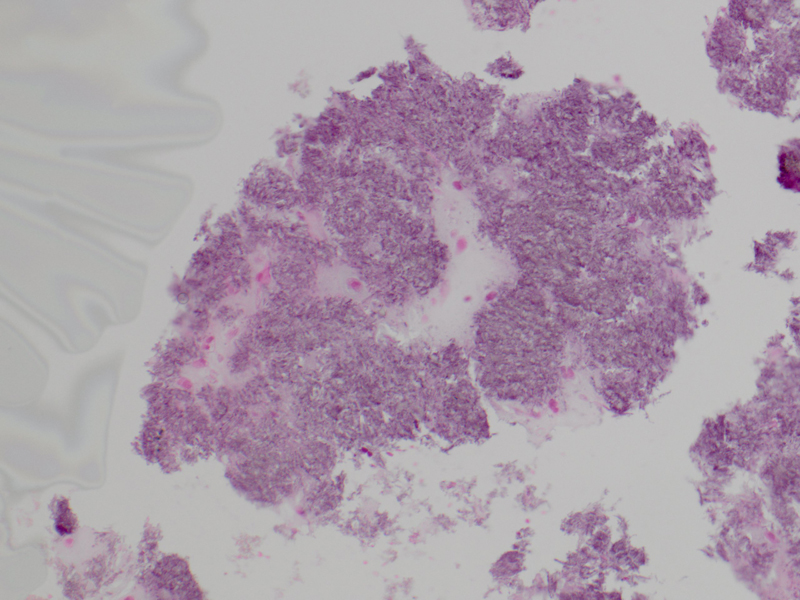
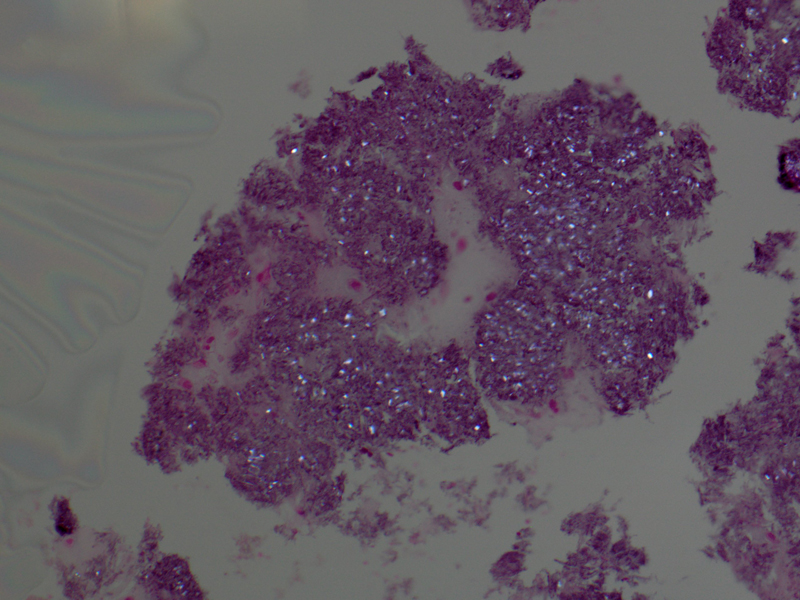
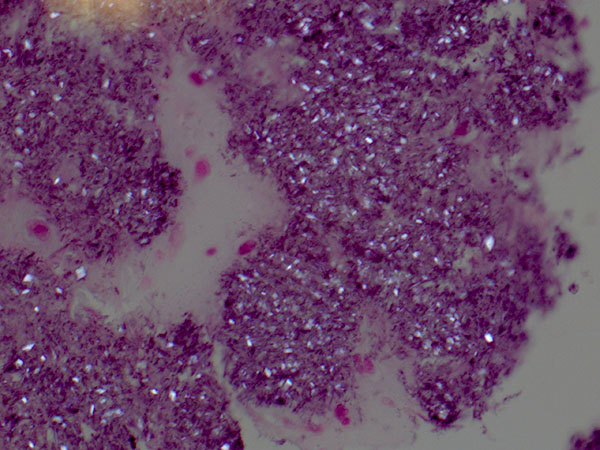
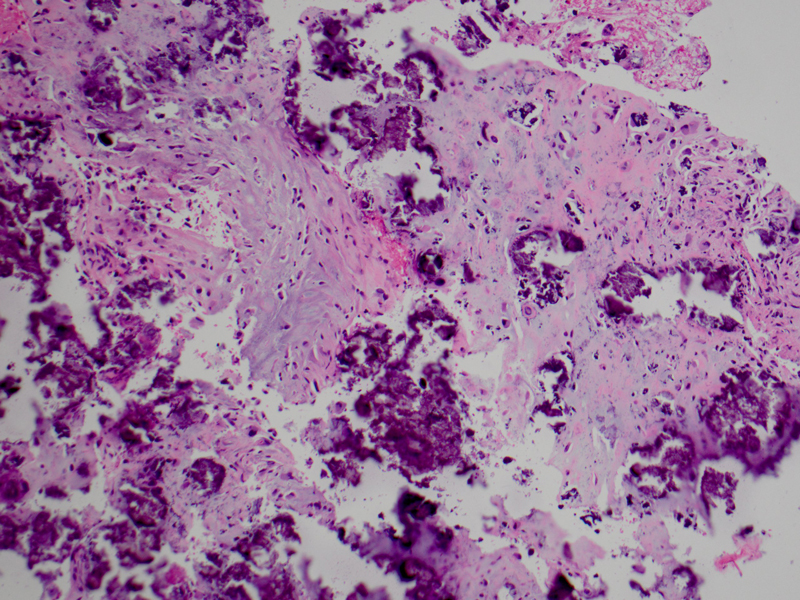
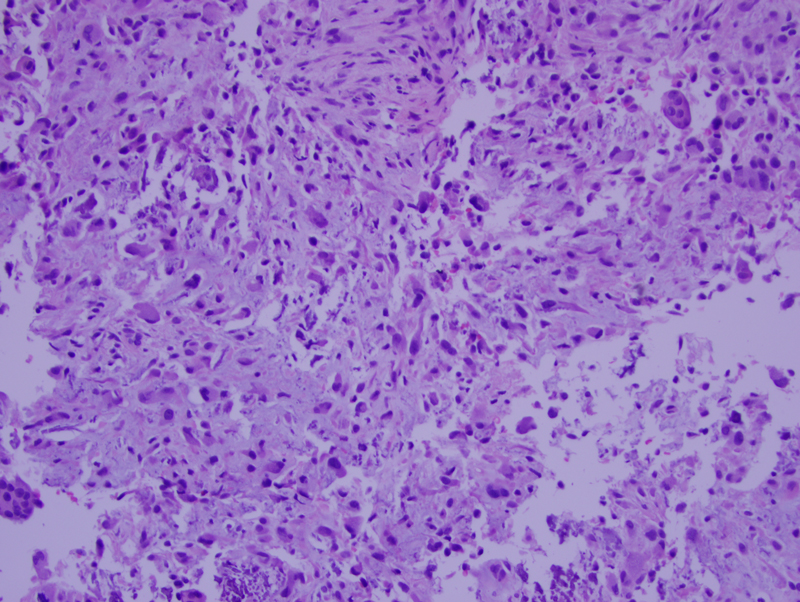
The biopsy specimen of the left skull base lesion demonstrated extensive basophilic calcifications with polarizable rhomboid shaped crystals consistent with calcium pyrophosphate dihydrate (CPPD) crystal deposits (Figures 3, 4, 5). The deposits are associated with reactive histiocytes and giant cells in addition to extensive chondroid metaplasia with atypia (Figures 6 and 7). The current biopsy was compared to the patient’s previous biopsy and appeared similar.