Case of the Month: Cough and Dyspnea
By Irene Chen, MD (PGY2), and Luis De Las Casas, MD
Clinical History
An elderly woman with past medical history of type II diabetes mellitus, hypertension, and anxiety, presented to the emergency department (ED) with worsening cough and dyspnea on exertion.
Recent History
In the ED, a chest x ray was done which showed bilateral pulmonary nodules that were not present on a routine chest radiograph a year prior. The subsequent chest computed tomography (CT) scan confirmed the presence of multiple bilateral solid pulmonary nodules, ranging from 0.3 cm to 1.2 cm in diameter. A subsequent positron emission tomography (PET) scan revealed that some of the nodules were mildly PET avid.
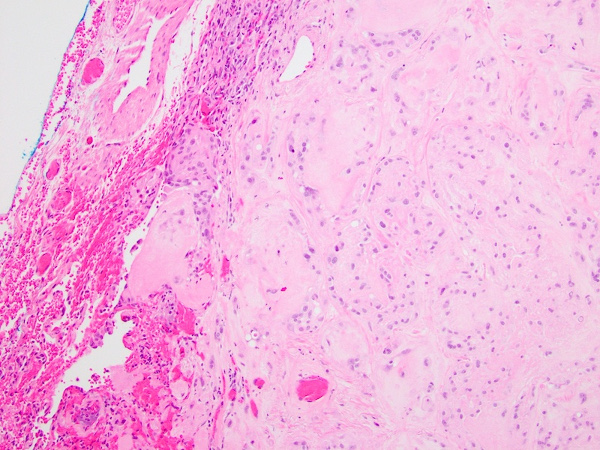
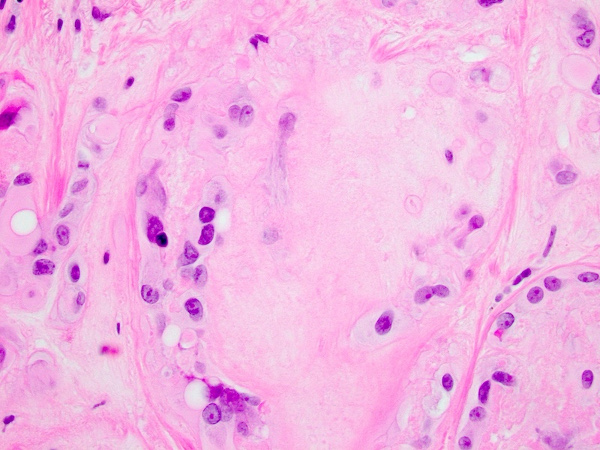
The patient underwent video-assisted thoracoscopic surgery of the right lower and upper lobes of lung. Gross examination of the resected specimen revealed two well-demarcated, intraparenchymal solid, round, white, firm tumors measuring 0.8 cm and 1.3 cm in greatest dimension. Microscopic examination revealed a well-circumscribed neoplasm composed of nests and cords of tumor cells within a myxohyaline stroma (Figure 1). The tumor cells had well-defined borders, abundant eosinophilic cytoplasm, and primarily round nuclei with open chromatin and conspicuous nucleoli (Figure 2). There were apparent cytoplasmic vacuoles in some of the neoplastic cells. No notable necrosis, mitotic activity, or nuclear pleomorphism was present.
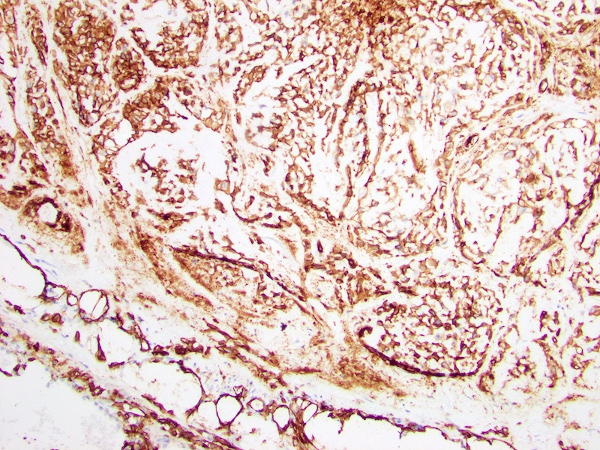
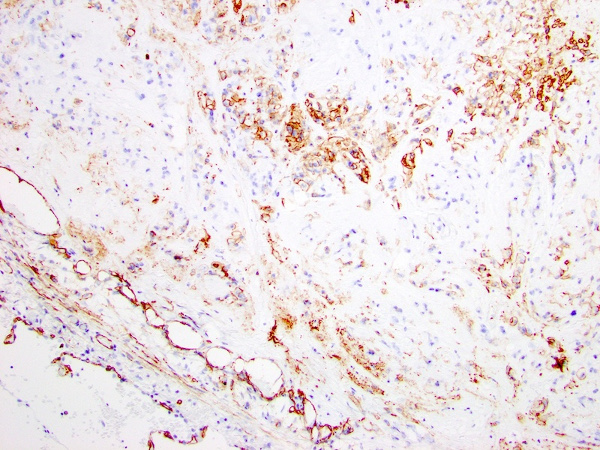
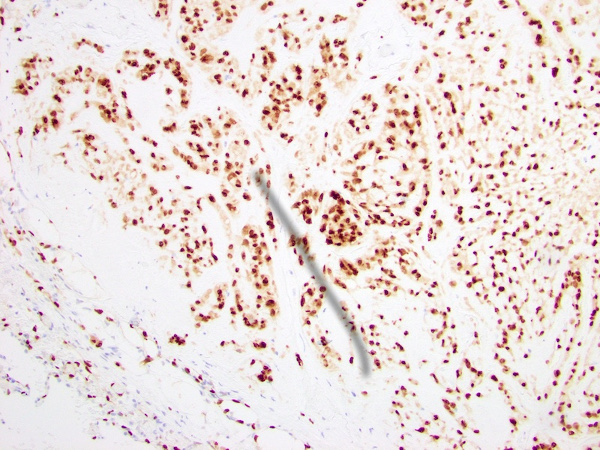
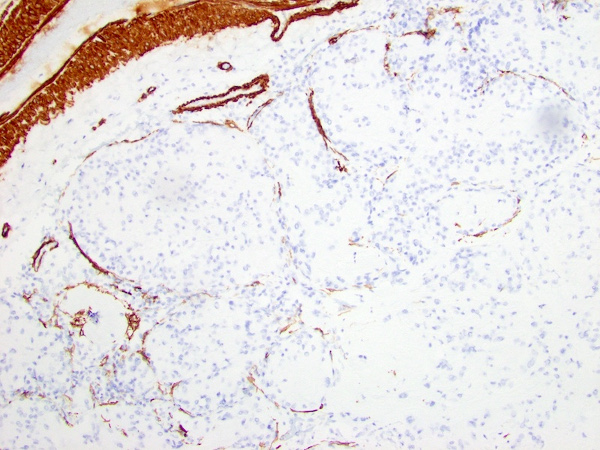
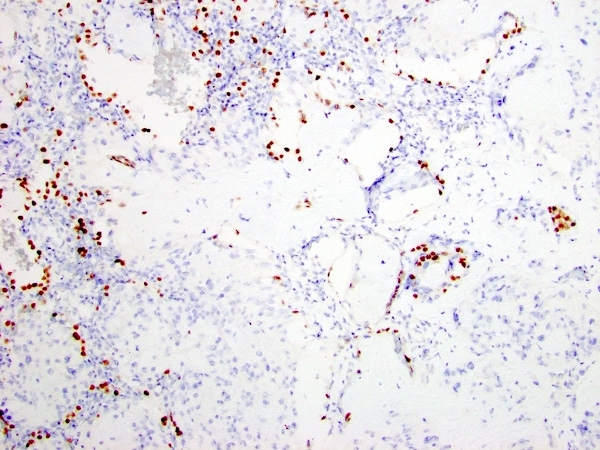
Immunohistochemical stains revealed that the tumor cells were positive for CD31, CD34, and ERG (Figure 3-5). The tumor cells did not mark with pancytokeratin, smooth muscle actin (Figure 6), epithelial membrane antigen, S-100 protein, HMB-45, SOX10, chromogranin, TTF-1 (Figure 7), PAX8, or desmin. No amyloid deposition was identified with Congo red stain.