Case of the Month: Splenic Lesion
Case authors: Dingani Nkosi, M.B.B.S., Ph.D. (PGY-1) and Walter Richard Burack, M.D., Ph.D.
Clinical History
A middle-aged man admitted for necrotizing alcoholic pancreatitis was found to have an incidental splenic lesion on imaging.
Past Medical History
His past medical history was significant for rheumatoid arthritis treated with adalimumab, polysubstance use, alcohol use disorder, chronic obstructive pulmonary disease and irritable bowel syndrome.
Recent History
His initial computed tomography (CT) scan showed a 4.3 cm hypoenhancing lesion in the spleen. Three months’ post admission, magnetic resonance imaging (MRI) revealed an increase in the size of the lesion to 6.9 cm. This was associated with weight loss, increased fatigue, early satiety and left upper quadrant fullness but the patient denied night sweats, fevers or any lymphadenopathy. A bone marrow biopsy showed nodular B cell aggregates and a clonal population of cells with immunoglobulin kappa light chain (IGκ) gene rearrangement consistent with small mature B cell non-Hodgkin lymphoma. The patient underwent a splenectomy for tissue diagnosis and for relief of some of his abdominal symptoms.
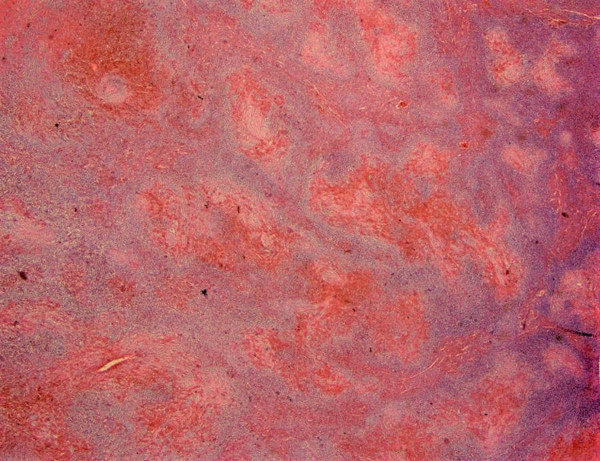
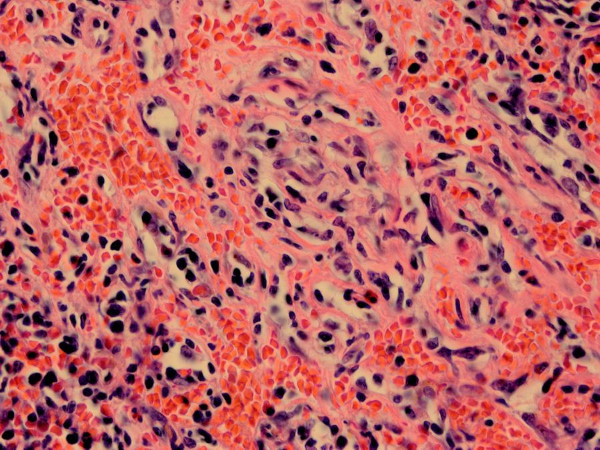
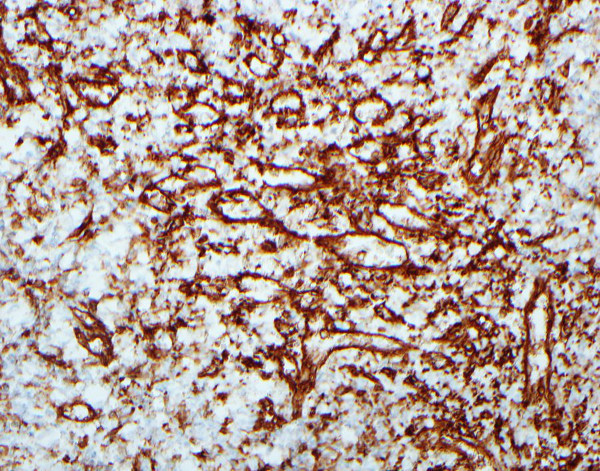
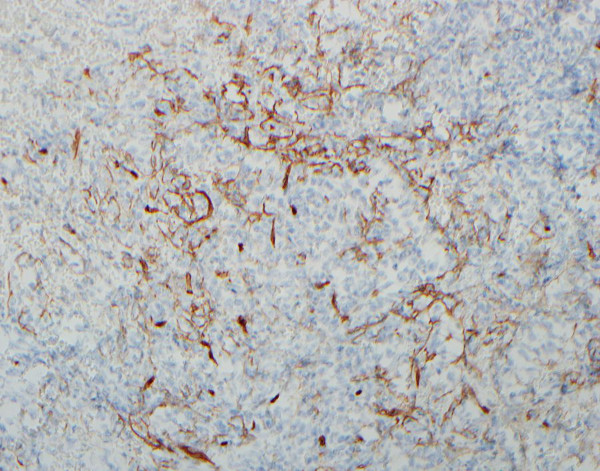
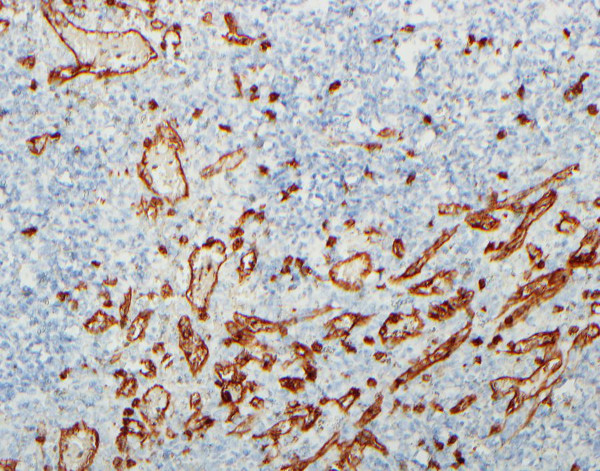
The spleen weighed 971 grams and measured 19 x 11 x 7.5 cm. The splenic capsule was nodular with scattered areas of subcapsular hemorrhage. Sectioning revealed a dark red, firm, homogeneous solid mass measuring 7.9 x 7.5 x 7 cm. On low magnification, there were unevenly distributed dark red nodules in various shapes and sizes surrounded by normal splenic parenchyma (Figure 1). Within the center of the nodules there were irregularly shaped small blood vessels lined by plump endothelial within a loose fibrous stroma and extravasated red blood cells (Figure 2). Immunostaining of the lesions showed positive staining for CD31, CD34 and CD8 (Figure 3-5). CD34 and CD31 highlighted the endothelium, while the CD8 highlighted littoral cells.