Case of the Month: Abdominal Skin Lesion
By Phoenix D. Bell, MD, MS, Kathleen Mannava, MD, and Aaron R. Huber, DO
Clinical History
A 70-year-old male with a past medical history of hypertension, gout, and hypothyroidism presents with a 3-4 week history of a rapidly-enlarging pustule on his left upper abdomen, which ultimately ulcerated (Figure 1).
Recent History
The patient also reports a 5-month history of intermittent substernal tightness, particularly after swallowing solid food. He denies decreased appetite, weight loss, fever, and chills, as well as nausea, vomiting, and diarrhea. The patient had a colonoscopy last year which showed one tubular adenoma and one sessile serrated polyp/adenoma.
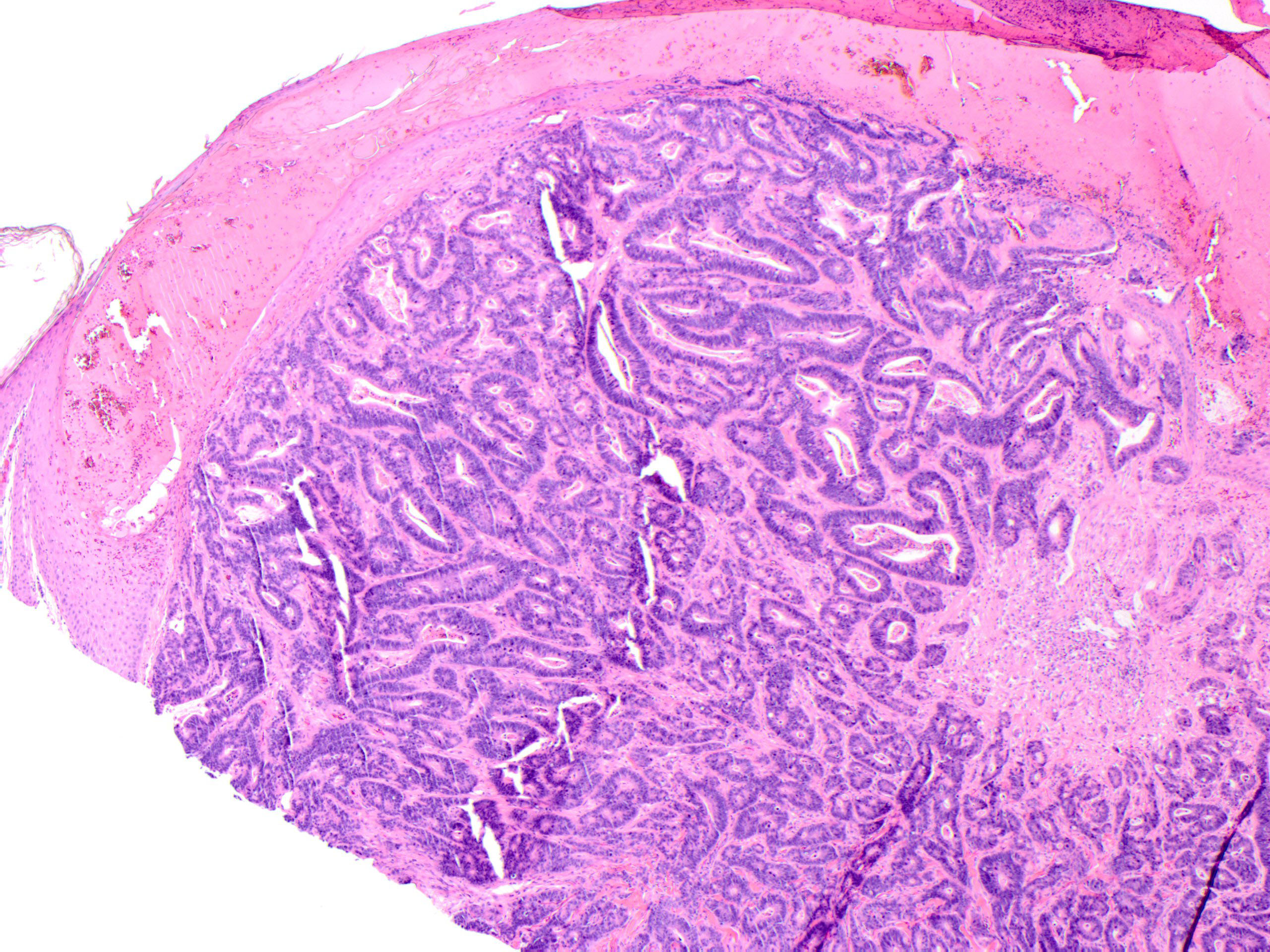
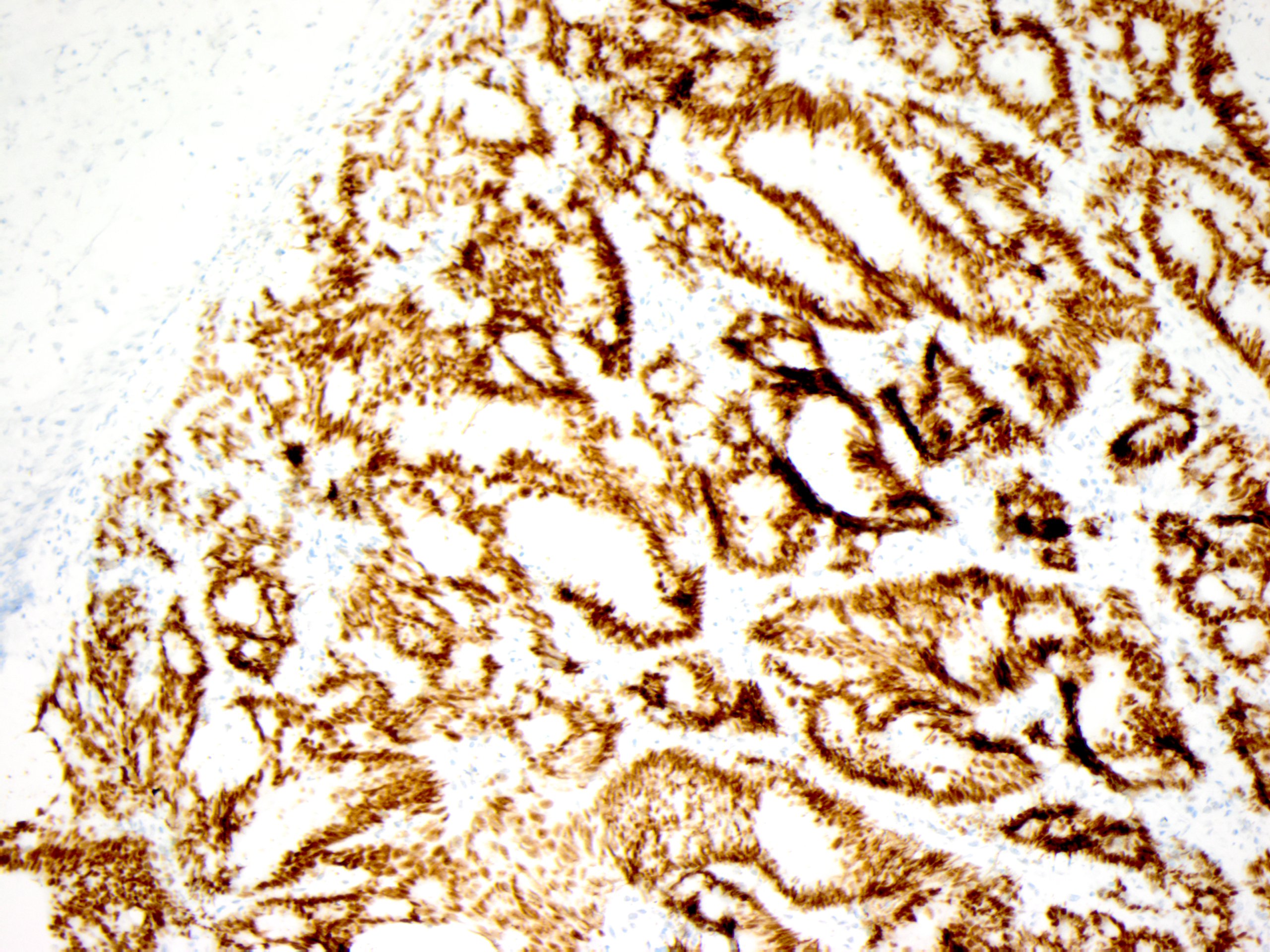
A biopsy of the skin lesion is performed and reveals squamous epithelium overlying a dermal-based infiltrative malignant gland-forming neoplasm composed of irregular glands (Figure 2). Immunohistochemical analysis reveals the cells of interest are positive for CK20 (Figure 3) and CDX2 (Figure 4), while negative for TTF-1 and PAX-8. The morphologic and immunophenotypic findings are consistent with a cutaneous metastasis from a gastrointestinal tract primary.
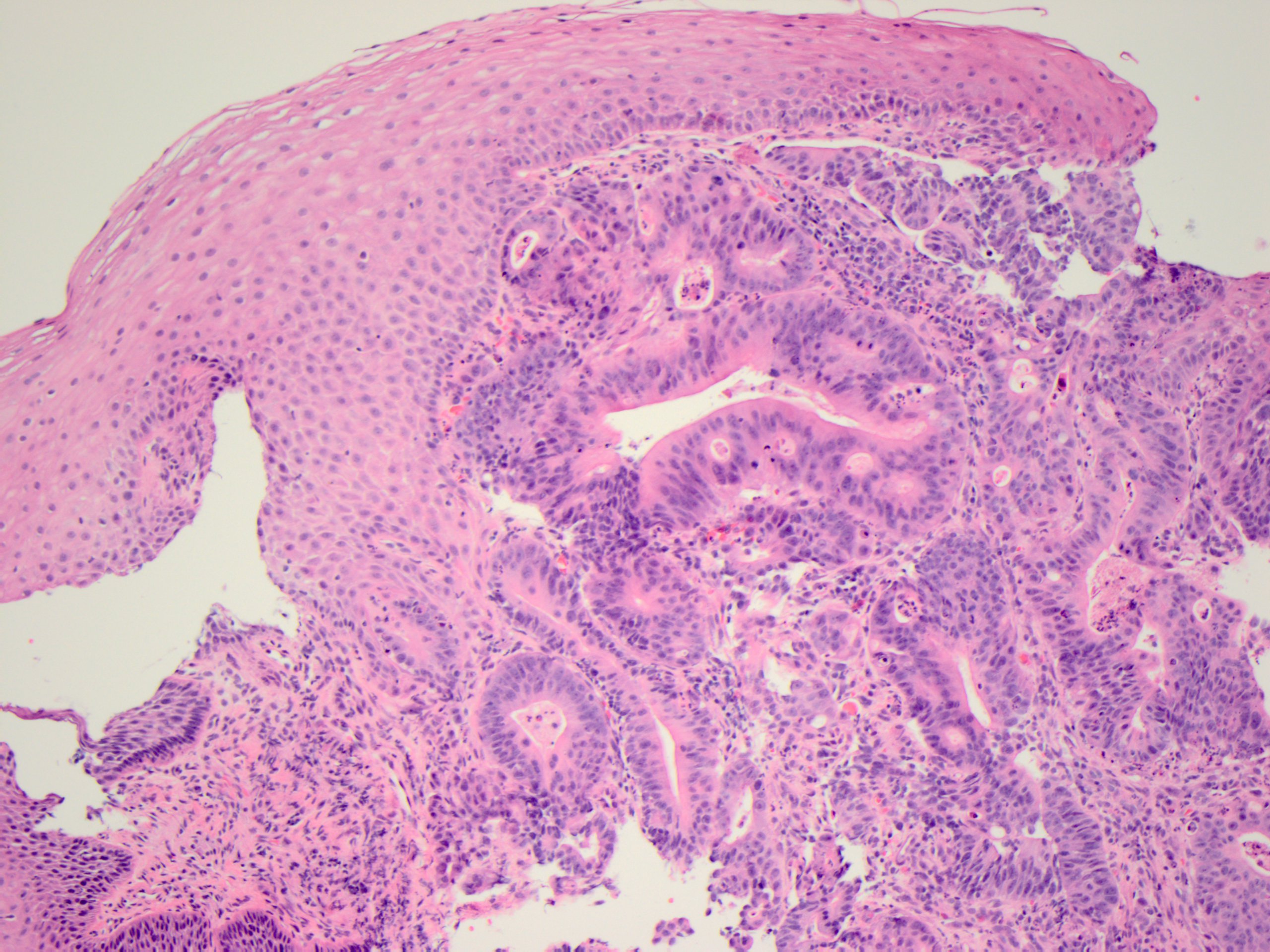
An abdominal CT scan is performed, which shows a heterogenously enhancing mass in the distal esophagus near the gastroesophageal junction. The patient is sent for an upper endoscopy, which demonstrates a partially occlusive 8 cm esophageal mass. Biopsy of this lesion shows a malignant gland-forming neoplasm undermining the squamous epithelium, morphologically compatible with the initial skin biopsy (Figure 5). The tumor cells also stain positive for CK20and CDX2 similar to the initial skin biopsy.