Case of the Month: Change in Bowel Habits
By Phoenix D. Bell, MD, MS, Larissa Temple, MD, and Aaron R. Huber, DO
Clinical History
A 75-year-old male with a history of aortic stenosis, hypertension, atrial fibrillation, chronic kidney disease, collagenous colitis, and celiac disease presented with a two-week history of watery diarrhea and several episodes of fecal incontinence.
Recent History
Given the history of collagenous colitis and recent worsening of diarrhea, the patient underwent a colonoscopy that demonstrated a large polyp involving the hepatic flexure, which involved multiple folds and approximately 50% of the circumference of the large intestine. Biopsies of the polyp revealed a tubular adenoma; however, it was not endoscopically resectable and a right hemicolectomy was performed.
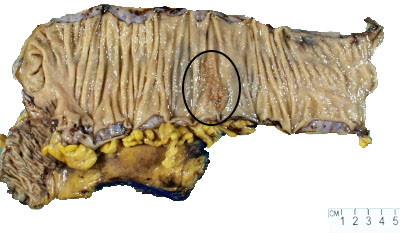
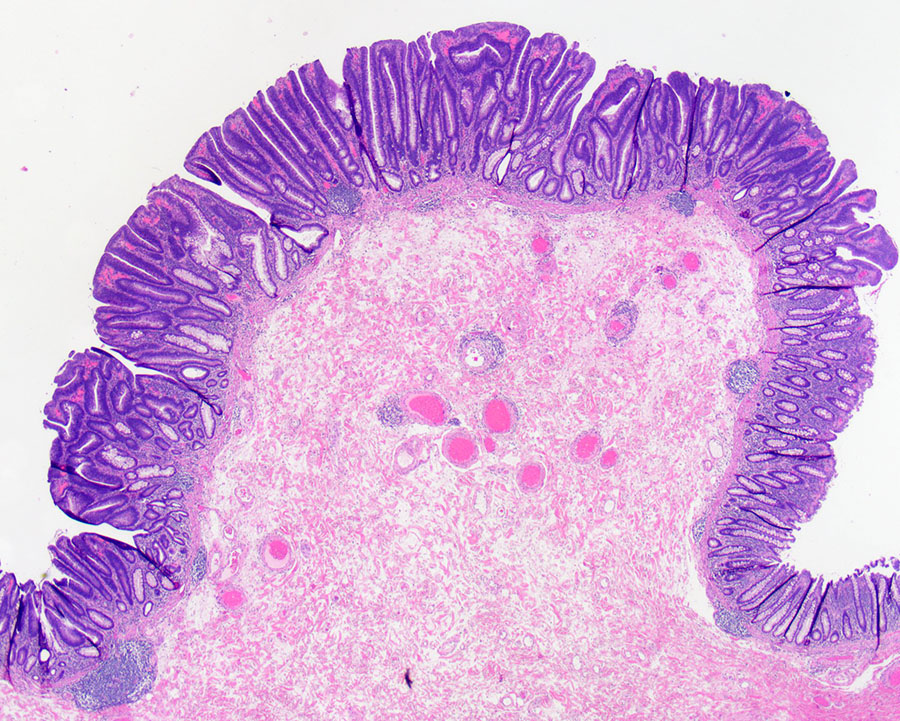
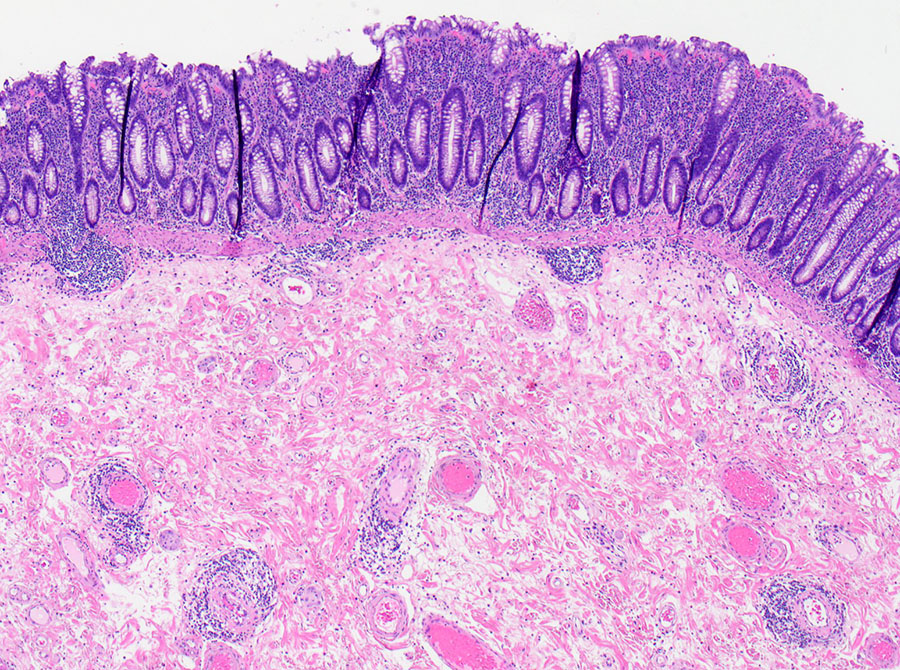
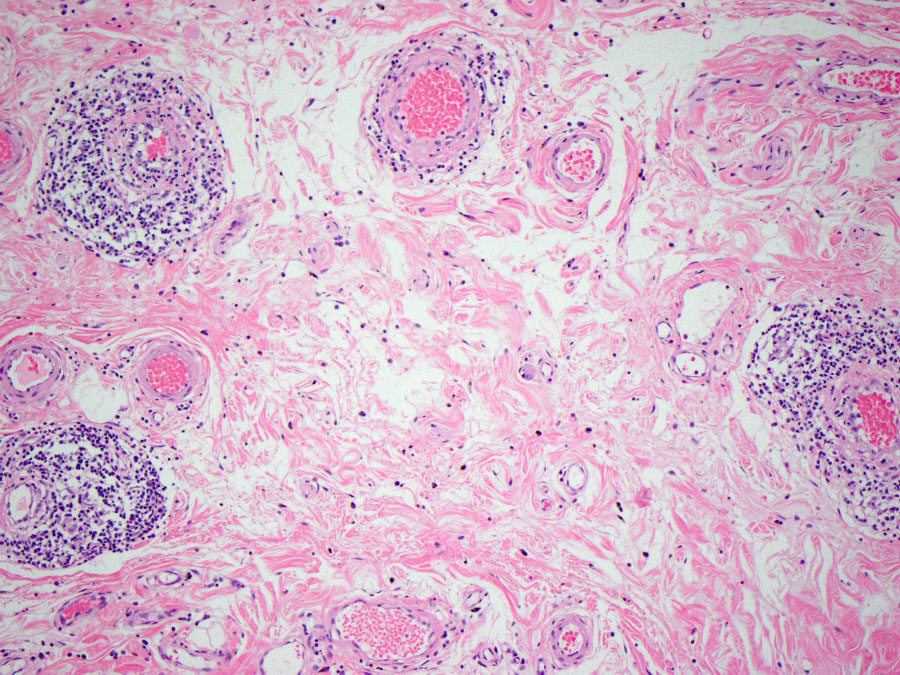
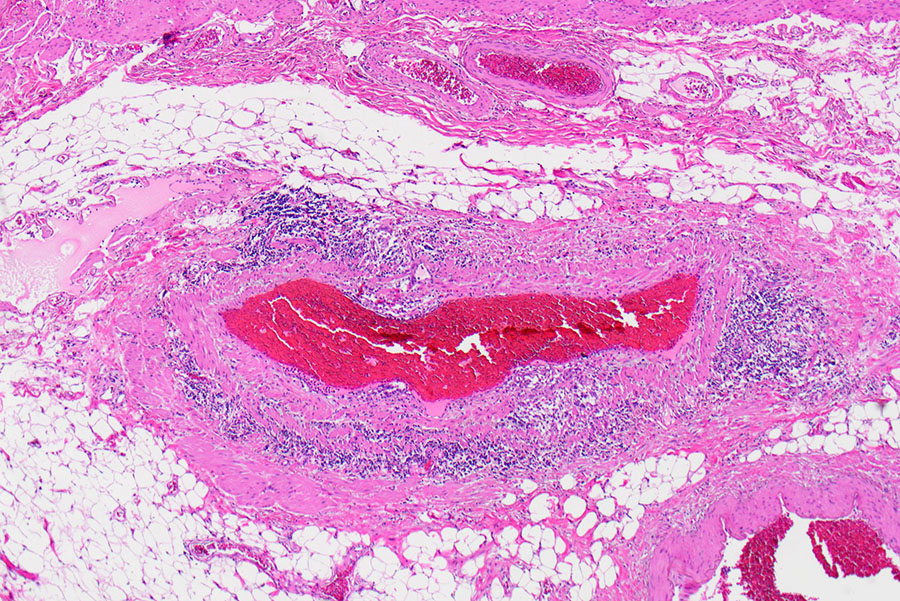
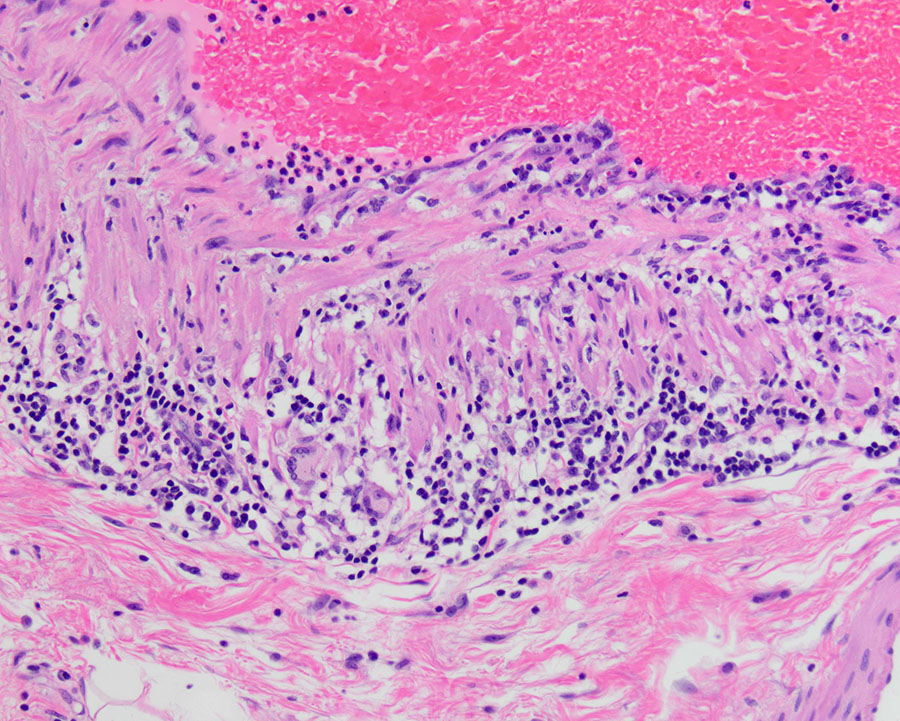
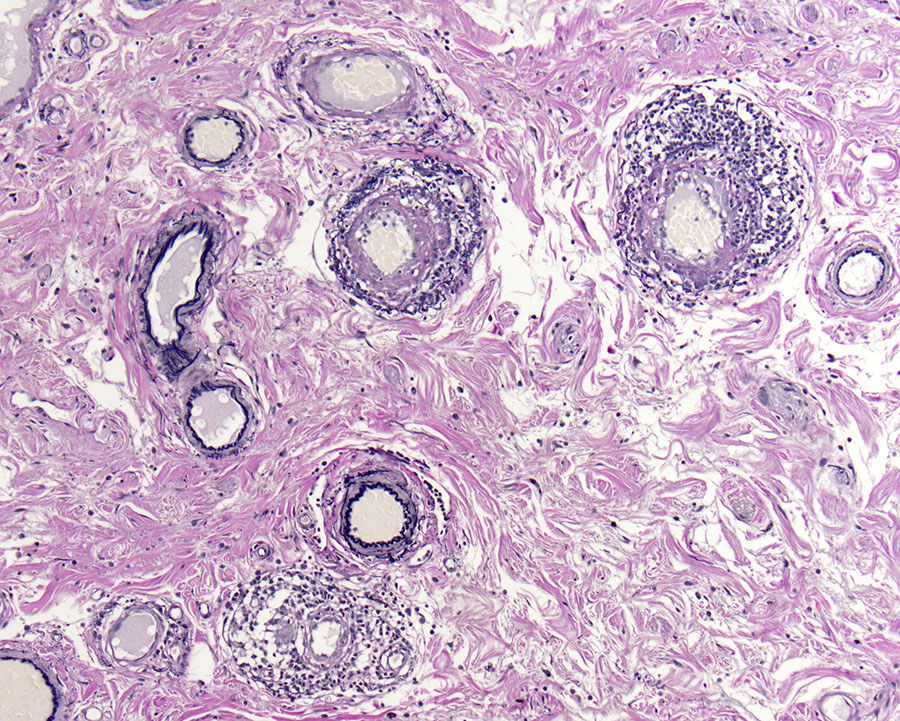
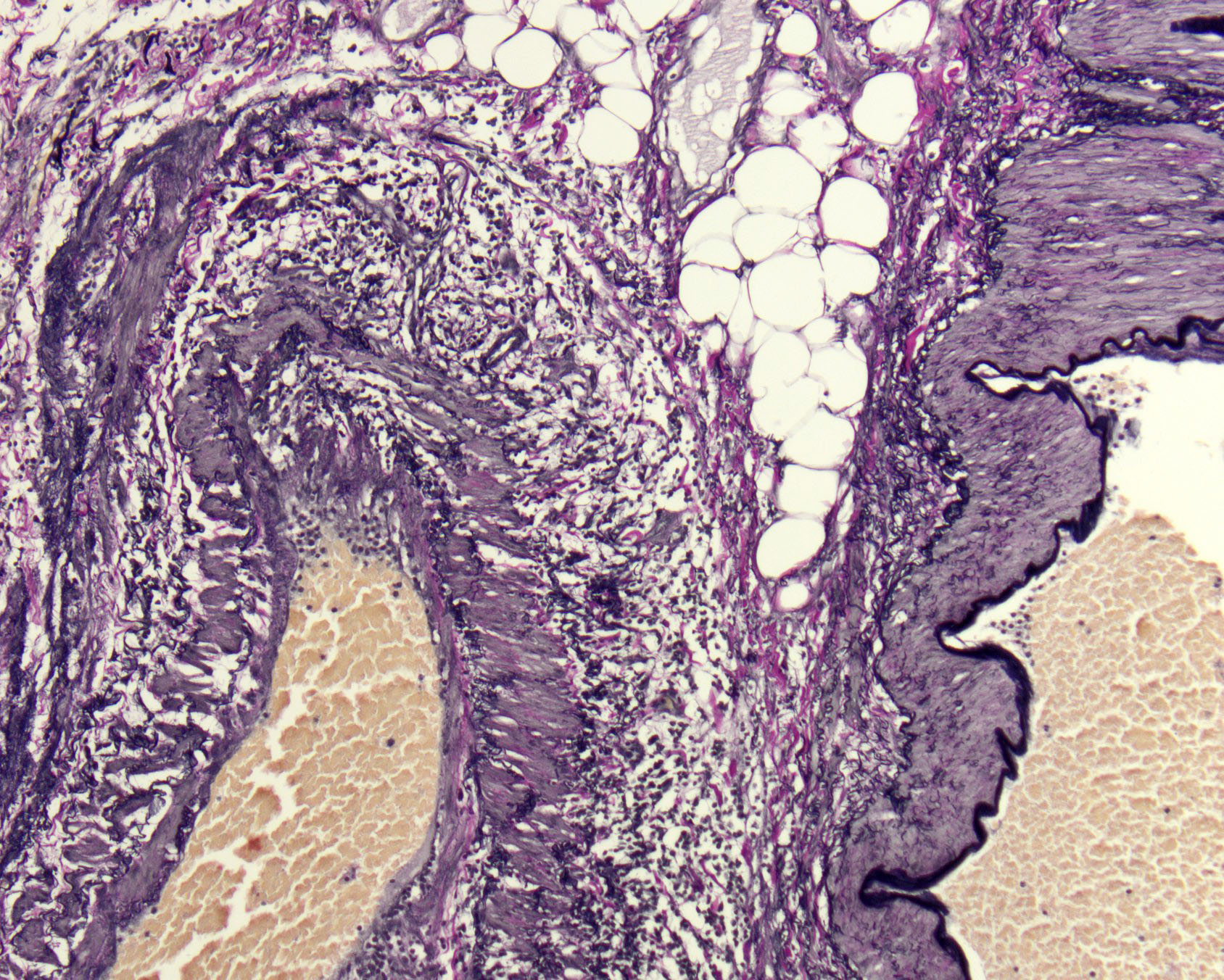
Gross examination showed a 4.7 cm pink-brown bosselated, polypoid sessile lesion involving the colonic mucosa (Figure 1). The polyp was entirely submitted and histologic sections revealed a tubular adenoma with no evidence of high-grade dysplasia or invasive carcinoma (Figure 2). Additional sections showed lymphocytic vascular and perivascular inflammation (Figures 3 & 4) with foci of inflammation containing epithelioid histiocytes and giant cells within the submucosa and subserosa (Figures 5 & 6). Elastic stains confirmed that the lymphocytic infiltrate was surrounding veins (Figures 7 & 8). Other microscopic findings included an increase in colonic and small bowel intraepithelial lymphocytes compatible with microscopic enteritis and colitis.